
Covid mRNA vaccine cancer risk
The study that keeps getting censored


As we have seen time and again during the Covid era, there are major barriers to publishing scientific work that is critical of Covid vaccines, with journals increasingly retracting papers for inappropriate reasons, or refusing to even send them out for peer review in the first place.
Add another paper to the pile: a recent preprint showing an association between increased excess cancer deaths and the modified-RNA (modRNA) Covid vaccine rollout has been retracted for the second time without good explanation.
Papers that get this treatment often contain important counternarrative insights, so I want to bring this study to your attention and unpack what it contributes to the growing body of knowledge on the modRNA Covid vaccines and their potential impact on cancer formation and mortality.
Index
modRNA Covid vaccines and cancer
The study: Correlation between excess cancer mortality and modRNA Covid vaccine rollout, Japan
How modRNA vaccines may contribute to cancer formation and mortality
Epidemiological association supports clinical evidence
The importance of biopsies in future research
A politically-motivated retraction?
Censorship of science highlighting Covid vaccine risks
modRNA Covid vaccines and cancer
For several years, experts in genomics and oncology have warned that modRNA Covid vaccines have the potential to pose a cancer risk.
While personnel at Australia’s Therapeutic Goods Administration (TGA) have privately acknowledged a theoretical cancer risk, regulators and health authorities have publicly dismissed concerns, counterclaiming that there is ‘no evidence’ of an increase in cancers caused by the modRNA Covid vaccines.
Regulators can say this because they did not require testing for carcinogenicity before approving these vaccines and, in Australia at least, the TGA is not monitoring cancer incidence as it was supposed to, nor does it attempt to determine the cause of adverse events, including cancers, reported to its safety surveillance database.
This leaves it to independent scientists to test the hypothesis that the modRNA vaccines could be causing cancer in vaccinated populations. This is especially important to people who already have cancer or who are in remission, as if modRNA vaccines do have cancer-promoting effects, then this risk needs to be weighed against any expected protective benefits.
While multiple potential mechanisms for cancer formation have been tabled, and case studies of rapidly developing cancers (colloquially called ‘turbo-cancers’) following modRNA vaccination have been documented, there has been scant epidemiological evidence, due mainly to the lag on national data reporting on cancer rates.1
The study: Correlation between excess cancer mortality and modRNA Covid vaccine rollout, Japan
However, a preprint from Japan showing an increase in excess cancer deaths temporally associated with mass modRNA Covid vaccination provides new population-level evidence of a potential modRNA-cancer link.
In the paper, ‘Excess Cancer Mortality after mRNA-Lipid Nanoparticle SARS-CoV-2 Vaccination in Japan: Observation until 2023,’ (Gibo et al., 2025) the scientists set out to analyse the impacts of the pandemic on cancer mortality, which is the leading cause of death in Japan.
With its large and relatively healthy population of 123 million and high levels of Covid vaccine coverage, the majority of which were modRNA vaccines, Japan is well-suited to this natural experiment.2 Figures were adjusted to account for Japan’s aging population.
The scientists found that while excess cancer mortality showed a gradual downward trend until 2020, a small but statistically significant increase of 1-2% emerged from 2021, continuing into 2023, in tandem with the Covid vaccine rollout.3 This is concurrent with a drop in life expectancy in Japan throughout the same period.
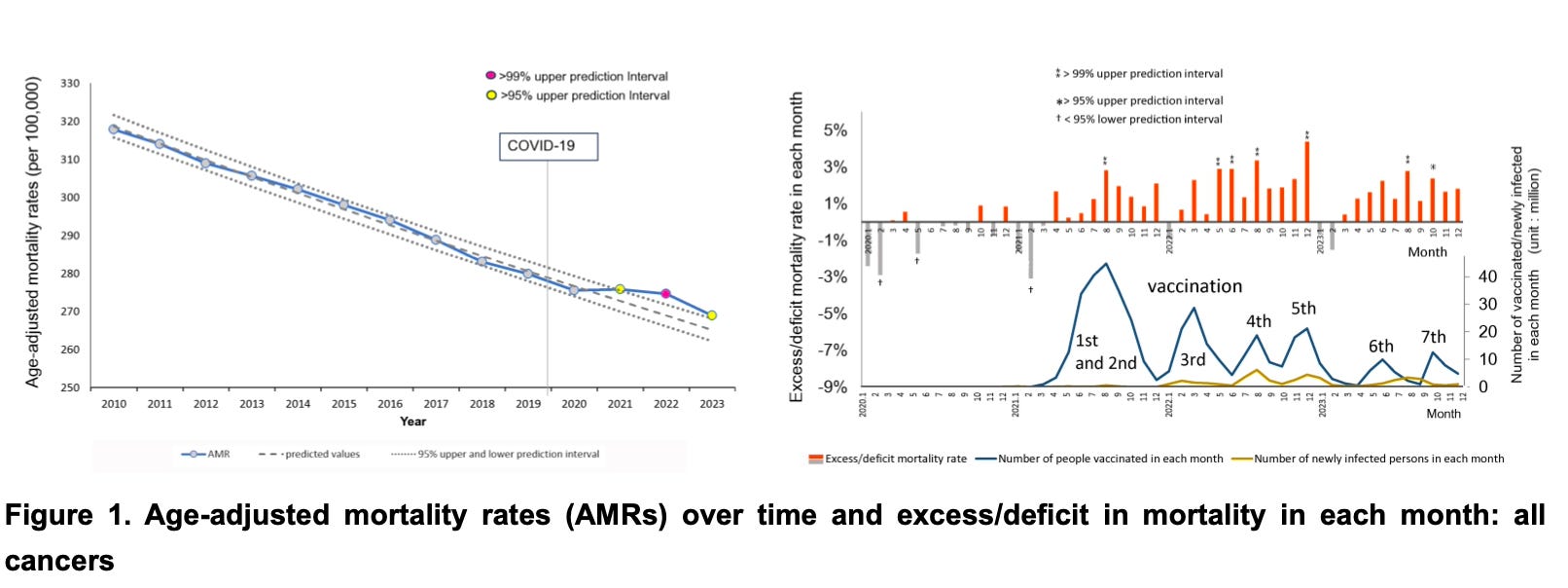
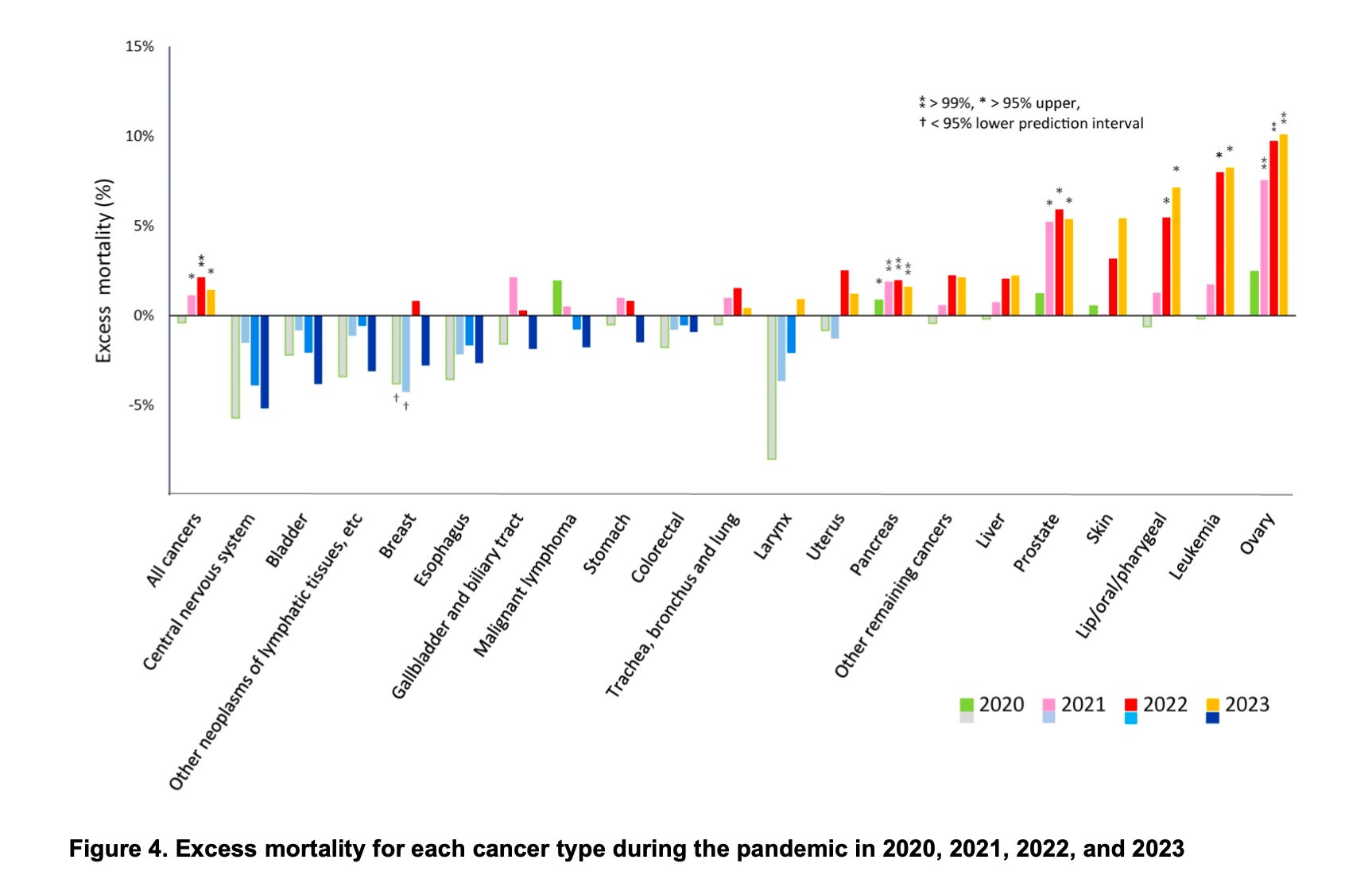
When broken into specific cancer types, the increase was much larger for certain types: ovarian, leukemia (blood cancer), lip/oral/pharyngeal, prostatic, and pancreatic. Of these, excess mortality from ovarian cancer and leukemia saw the largest annual increases at 10% and 8% in 2022 and 2023, respectively.
While excess cancer mortality was most pronounced in older age groups, which were more heavily vaccinated, the scientists found a statistically significant signal in those as young as 50.
The authors were careful to articulate that “the causal relationship between excess cancer deaths and large-scale vaccination cannot be assessed in this study,” but that “the coincidence of timing might require further research.”
One of the most unsatisfactory elements of Covid-related studies to date has been the failure oftentimes of scientists to consider the impact of Covid vaccines and infections, or to mount an argument for why they think one factor more likely explains their findings than the other.
In this study, the scientists discussed a range of potential drivers of the increase in excess cancer mortality, estimating the impact, for example, of missed cancer screenings due to lockdowns that may have accounted for some cancer deaths in 2020.
On the impact of Covid infections vs mRNA vaccines, the authors noted,
“The cumulative number of vaccination doses given up to the end of 2023 (436 million) was nine times the number of newly confirmed infections (47 million), suggesting that the vaccine may have had a greater impact on the Japanese population than the infections themselves."
How modRNA vaccines may contribute to cancer formation and mortality
The authors then discussed potential mechanisms for cancer formation and mortality arising from modRNA vaccines to test whether a causal link between excess cancer mortality and the vaccine rollout is plausible (some additional details under the authors’ headings have been added by me).
The effects of multiple modRNA Covid vaccine doses
The authors highlight that the cumulative effect of repeat vaccinations on top of infections should be considered, as this increases exposure to certain risk factors. Remembering, as at the end of 2023, the Japanese population had been exposed to nine times as many shots as it had infections.
Vaccinations increase exposure to the spike protein, in terms of incidence (per shot), amount, and persistence (up to two years), and target organs that may not otherwise accumulate large amounts of the spike protein (via pro-inflammatory lipid nanoparticles [LNPs]).
Over the medium-to-long term, modRNA Covid vaccines have demonstrated negative efficacy, meaning that more highly vaccinated individuals are more prone to infection than less or unvaccinated individuals. This further exacerbates exposure risk.4
Thrombogenic effects of spike protein and LNP
Because cancer often leads to coagulation (blood thickening and clotting) via various mechanisms, one of the major causes of mortality in patients with cancer is cancer-associated thrombosis (blood clotting that blocks a vein or artery).
Studies show that the spike protein has various pro-coagulation and inflammatory effects. Therefore, the risk of thrombosis increases with both modRNA vaccinations and Covid infections in individuals with cancer.5
Suppression of cancer immunosurveillance
Suppression of cancer immunosurveillance essentially means that your body is less likely to identify and repair damaged DNA pathways, allowing for cancer growth.
Studies show that modRNA Covid vaccines can suppress cancer immunosurveillance due to impacts on type I interferon (IFN) responses, BRCA2, PD-L1, p53 and IgG4.6
Possible effects of spike protein on development and progression of specific cancers
In this study, mortality for ovarian cancer, leukemia, lip/oral/pharyngeal, prostatic, and pancreatic cancers were in excess beyond the predicted rates from 2021 to 2023 by a statistically significant margin. These are estrogen- and estrogen receptor alpha (ERα)-sensitive cancers; research shows spike protein impacts on ERα.
If spike protein enters the cell nucleus - and there is evidence that it can - it can disrupt DNA repair pathways involving BRCA1 and 53BP1. Associated cancers include breast, uterine, and ovarian cancer in women, prostatic cancer in men, and pancreatic cancer and acute myeloid leukemia for both men and women.
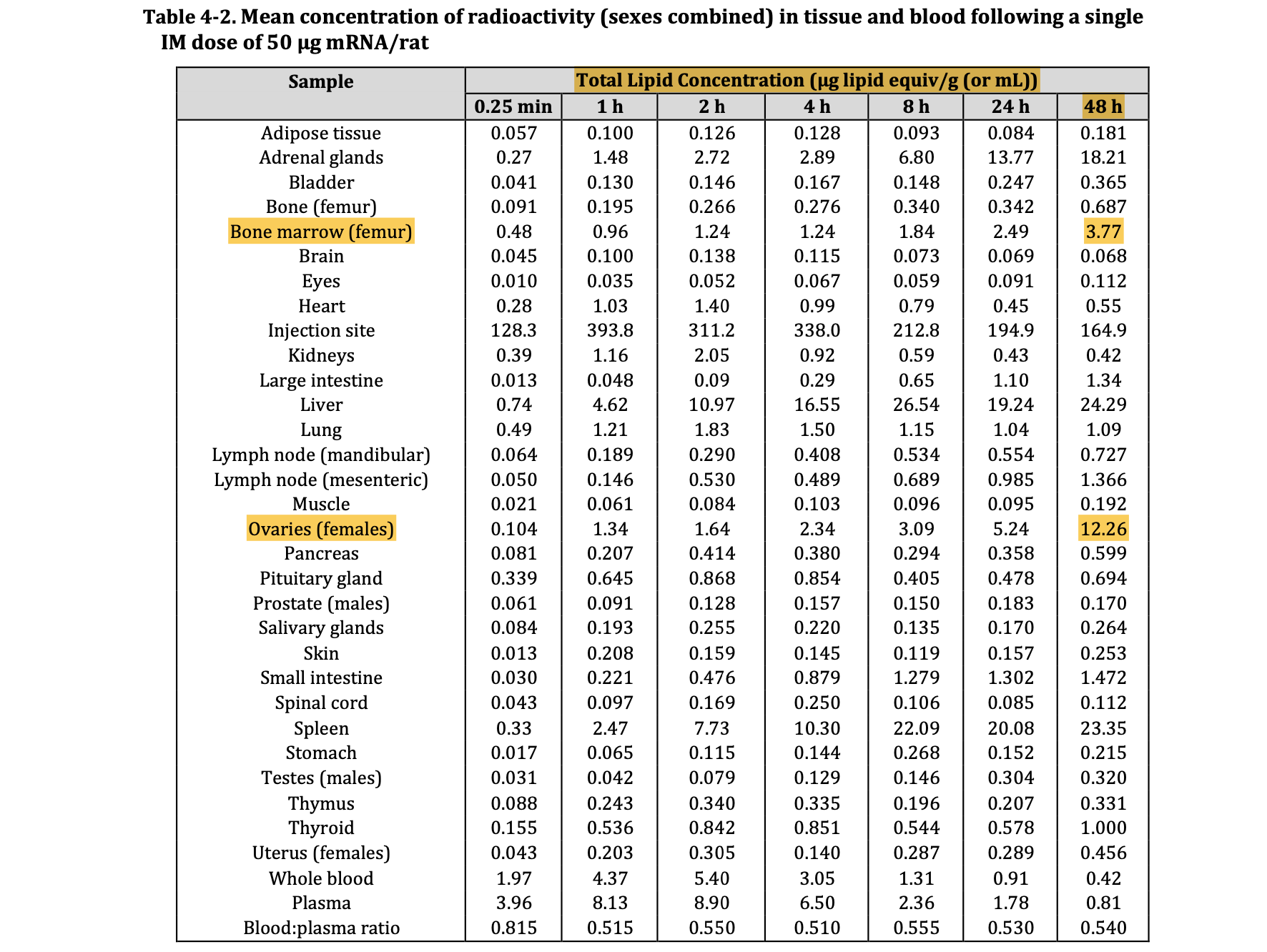
As LNPs accumulate particularly in the ovaries and bone marrow, this could explain findings of excess mortality for ovarian cancer and leukemia, which are estrogen-sensitive and may be influenced by the spike protein.7

Distribution and concentration of LNPs in rats up to 48 hours post-injection with Pfizer COMIRNATY vaccine, Pfizer Nonclinical Evaluation Report January 2021, FOI 2389 document 6.
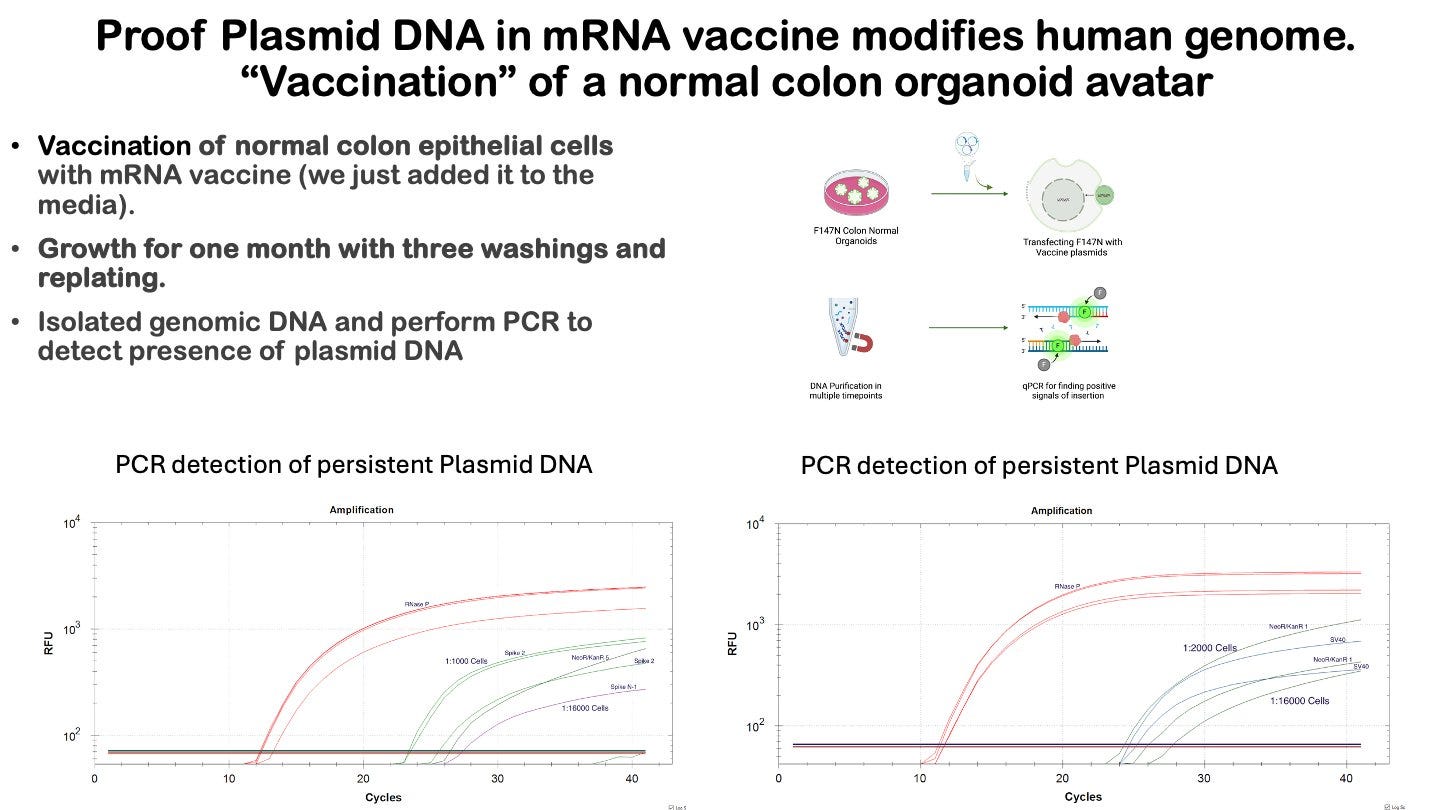
Residual synthetic plasmid DNA fragments
DNA contamination at levels above the regulatory limit of 10 nanograms (ng) per dose have been repeatedly identified in independent labs and recently in one of the Food and Drug Administration’s (FDA) own labs.
LNPs deliver this contaminant DNA directly into cells (a process called ‘transfection’), whereas in traditional vaccines, it is more likely that contaminant DNA will be destroyed by the body soon after injection. Therefore, current regulatory limits for contaminant DNA in vaccines may be irrelevant (too high) for new LNP vaccines.
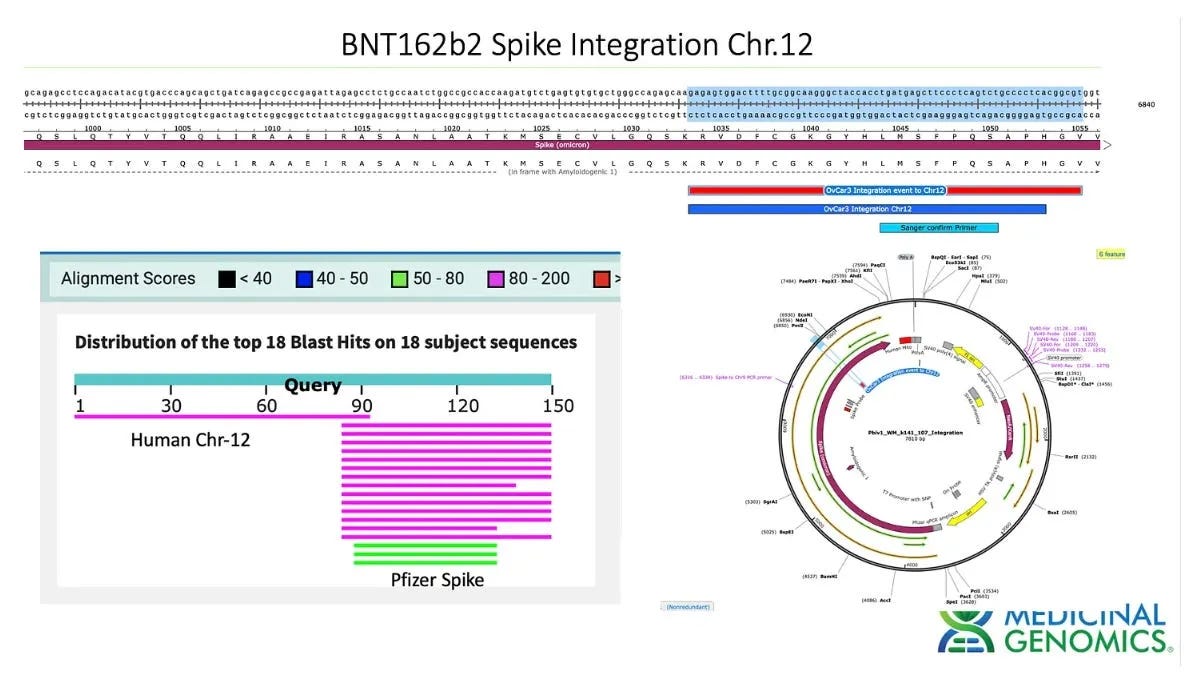
The FDA states in its guidance for industry, “There are several potential mechanisms by which residual DNA could be oncogenic, including insertional mutagenesis following DNA integration.”
In the Pfizer vaccine, the SV40 enhancer/promoter gene therapy sequence is also present, heightening oncogenic risks due to its efficiency at dragging materials into the cell nucleus and its impact on p53 (a tumor suppressor gene).
Even in the absence of integration into the genome, cGAS–STING signaling induced by the presence of foreign DNA in the cells is reported to have a tumour-promoting function.8
Epidemiological association supports clinical evidence
Oncologist and melanoma immunotherapy specialist Professor Angus Dalgleish said that the Japanese findings fit with the picture he is seeing in his clinical experience in terms of the coincidental timing following vaccination, the types of cancers, and the age of patients.
Over email, Professor Dalgleish told me that he saw “an increase in relapse of melanomas after the third [booster] vaccines were rolled out,” as well as increases in all types of cancer more generally, especially pancreatic, colorectal, ovarian, and gliomas (cancer of the brain or spinal cord) after the boosters.
“My colleagues have seen an excess in other tumour types occurring at later stages and in younger people,” he added.
Furthermore, “My own research has shown that the boosters suppress the T-cell response and switch the antibody response to tolerising,” Professor Dalgleish said in a video statement prepared for a special meeting of the Port Hedland Council last year relating to DNA contamination concerns.
“That means this is the perfect example where you have switched off the policing of foreign invaders, virus, etcetera, and cancer, allowing it to grow uncontrolled,” he said.
Excerpt from Professor Dalgleish’s address to the Town of Port Hedland, 11 October 2024 (Clip 2:26 mins). Source.
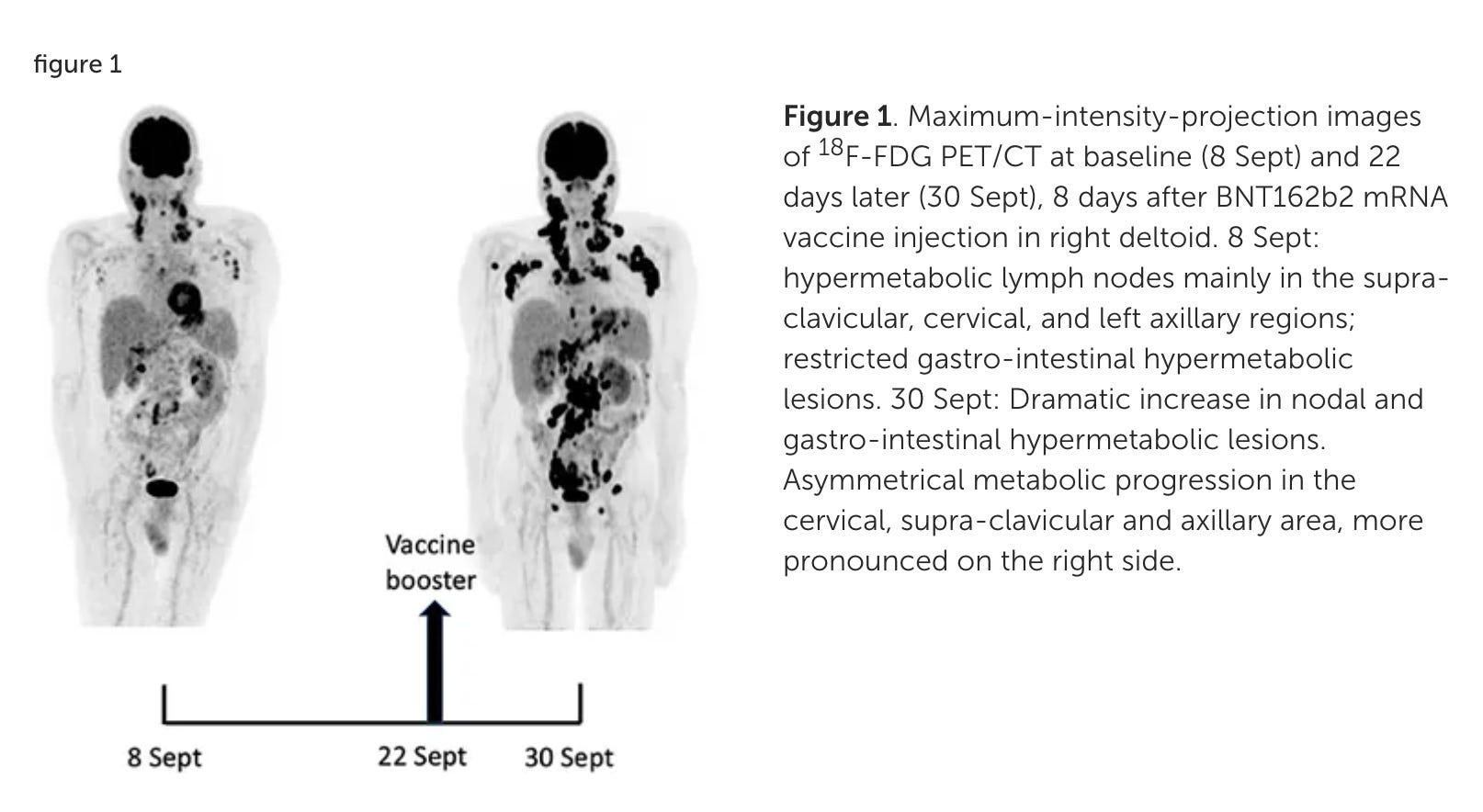
Professor Dalgleish is not alone among highly credentialed doctors with compelling accounts of turbo-cancers. Most famously, Belgian immunologist Michel Goldman became the subject of his own case report when his lymphoma rapidly progressed after a modRNA booster, exploding into “so many spots that it looked like someone had set off fireworks inside Michel’s body.”
In the peer-reviewed report ‘Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot’ (2021), Goldman and his co-authors discussed the possibility that the Pfizer vaccine’s “potent stimulation of T follicular helper (TFH) cells” induced the progression of his cancer. ‘T cell exhaustion’ is another form of dysfunction to the tolerising effect, both of which have been raised by Professor Dalgleish.
The pattern of spread and the “dramatic speed and magnitude of the progression” were further evidence supporting this hypothesis. The cancer appeared to be most concentrated initially on Goldman’s left side, the same side on which he received his first two vaccinations. However, after the booster shot in Goldman’s right deltoid, there was a “dramatic increase” in cancer lesions, particularly on the right side.
While Goldman remains a committed proponent of modRNA vaccines, Professor Dalgleish has taken a more precautionary approach, raising the alarm about the potential oncogenic risks of the mod-RNA vaccines and calling for better research and surveillance.
“There must be an urgent study to measure spike proteins in patients who have been vaccinated with more than two vaccines, and correlate the presence with cancers as well as compulsory inspection of all cancers for spike mRNA incorporation,” he said.
“I have tried to do this in the UK but the National Health Service (NHS) have virtually banned such studies even when funded! Why, why, why???” he added, expressing frustration at health authorities’ lack of interest in this issue.
The importance of biopsies in future research
Testing of human tissue samples has produced early evidence of integration of contaminant DNA with human cell DNA. If replicated under rigorous conditions, this will have major implications for cancer formation, as DNA integration can disrupt genome stability, leading to mutations, altered gene expression, and uncontrolled cell growth.
Genomics scientist Kevin McKernan, who initially discovered the high levels of DNA contamination and the presence of the SV40 enhancer promoter in the Covid modRNA vaccines, has been at the forefront of testing tissues for integration, along with cancer genomics scientist Dr Phillip Buckhaults.
McKernan, along with German molecular biologist Dr Ulrike Kämmerer, identified Pfizer vaccine contaminant DNA in ovarian cancer cell line DNA in lab testing last year, and is doing further work to see if the results are replicable.
Over email, McKernan told me that DNA sequencing of human cancer tissues is essential to figuring out whether there really is a causal link between modRNA vaccines and cancer development.
“We need to be qPCRing every post-vax biopsy and perform deep sequencing on those positive samples,” he said.
“[Ethics approvals] are finally in place and this is beginning to happen.”
We also need to screen the blood supply, said McKernan, referring to findings of modRNA Covid vaccine DNA contamination in blood samples from South Australia. “How much of this is transmissible through blood banks?”
A politically-motivated retraction?
The preprint discussed in this article is the second iteration of a peer-reviewed study published in April 2024 in the journal Cureus (part of Springer Nature), and retracted the following June after the Director of Publishing contacted the authors citing a Reuters ‘fact check’.
The article went ‘viral,’ being viewed approximately 287,000 times in the first three months following publication, and prompting many online news articles (it has now been viewed over 329,000 times).
The Reuters fact check claimed that the study, which had passed through the rigorous peer-review process, was “flawed” based on the opinion of just one professor who appears to have misunderstood the study (you know how I feel about the fact-checker con).
The authors replied strongly arguing against the retraction and meticulously rebutting the Reuters article. However, Cureus proceeded with the retraction because “the correlation between mortality rates and vaccination status cannot be proven with the data presented in this article.”
To be clear, the authors never claimed to prove a correlation between mortality rates and vaccination status, but rather highlighted a correlation between mortality rates and the population-wide vaccination rollout.
Undeterred, the Japanese scientists added an extra year’s worth of vital statistics data, beefed up the section on DNA contamination as a potential contributing factor, and finessed the language to make it abundantly clear that they are not claiming to have proven a causal link between modRNA Covid vaccines and excess cancer mortality.
The revised paper, called 'Excess Cancer Mortality after mRNA-Lipid Nanoparticle SARS-CoV-2 Vaccination in Japan: Observation until 2023,' was uploaded to the preprint server Zenodo in February. Within weeks, it had been taken down.
First author Dr Miki Gibo said that the authors had “no idea” why their paper had been taken down as they received no retraction inquiry or notice from Zenodo regarding its removal.
However, a representative for Zenodo responded to my email inquiry advising that the preprint was removed from the server because it is “almost identical” to the version retracted by Cureus.
“Our standard practice as a repository (a digital archive for scientific research outputs) is that if a journal retracts a paper we also retract the paper from Zenodo,” said the representative.9
The authors are now pursuing peer review and publication with a journal that does not receive funding from the pharmaceutical industry, unlike Cureus (and most major journals), which receives an undisclosed amount from the industry in advertising and sponsorship spending.
Censorship of science highlighting Covid vaccine risks
The retractions of the Japanese cancer mortality research follow a familiar pattern. A peer-reviewed paper highlighting risks associated with Covid vaccines is published. It garners widespread attention because such papers are a rarity, and they provide scientific evidence or explanations for what people are observing anecdotally.
The virality of such papers draws the attention of fact-checkers and journalists who publish articles discrediting the paper, after which it is swiftly retracted by the journal/publisher under strange circumstances, sometimes without adherence to publishing ethics guidelines.
This is more or less exactly what happened to a peer-reviewed paper highlighting that the spike protein from both the SARS-CoV-2 virus and the associated vaccines caused damage to key DNA repair pathways, with implications for cancer formation (Jiang and Mei, 2021).
A years-long investigation by multiple parties eventually revealed that the retraction was a sham, motivated not by scientific integrity, but by pressure from fact-checkers and hysterical pro-vaccine sentiment.
EXCLUSIVE REPORT: Forced retraction of Covid vaccine cancer-risk study, scientist alleges

New evidence uncovered in a two-years-long investigation reveals that one of the authors of a retracted paper revealing the Covid vaccines’ potential to cause cancers never agreed to its retraction, which she now claims was “forced” in “violation of academic ethics.” Emails obtained under FOIA corroborate her story.
There are more:
A study of myocarditis cases reported in teenagers to the VAERS database after Covid vaccination was retracted by publisher Elsevier just days after publication. After being reworked, peer-reviewed, and finally republished in January 2024, the revised paper is now being required to undergo ‘post publication review’ over a year later.
A survey study estimating nearly 300,000 Covid vaccine deaths in the US in the first two years of the rollout was retracted after an intense media campaign against the paper, leading to its retraction and the author, Dr Mark Skidmore, being subjected to an ethics review at his university. The paper, which remains in the top 1% of papers published worldwide, has since been republished.
A review of Covid modRNA vaccine trial data and post-injection injuries, a post-marketing safety study of Covaxin, and multiple papers by gastroenterologist Dr Sabine Hazan are further examples of scientific research retracted on flimsy grounds.
More recently, journals’ role as gatekeepers preventing the publication of counternarrative science was highlighted by the repeated rejection of a study on DNA contamination in the modRNA shots by high-impact journals, which refused to even send it out for peer review.
“Is the relationship between mRNA products and cancer so bad for pharma, Ellison, Sun, and others who are insisting on cancer mRNA therapy while increasing cancer?” mused Gibo, referring to the new Trump administration’s recent hype around using AI to inform development of modRNA therapeutics for cancer.
It is probably not lost on the authors, or on readers, that companies heavily invested in modRNA vaccines also have interests in cancer research and therapeutics - such as Pfizer’s acquisition of cancer medicine firm Seagen and Moderna’s development of modRNA cancer vaccines.
Neither is Trump alone in backing modRNA technology all the way - in Australia, federal and state governments are partnered with universities and with modRNA research, development and manufacturing companies, pegging the success of our economy and biomedicines industry to the success of modRNA technology. Same story in the UK, and worldwide.
In an email, Gibo praised the efforts of the Port Hedland Council and other local governments to bring the potential cancer risk of the modRNA to the attention of federal and state authorities.
“We hope Australia's courageous local authorities will succeed in the world's first fight as local government against the mRNA vaccine,” she said.
With ongoing censorship of critical scientific findings, it’s an uphill battle.
To support my work, share, subscribe, and/or make a one-off contribution to my Kofi account. Thanks!
Further reading
Research showing modRNA Covid vaccines may increase the risk of the development and progression of cancer, Gibo et al. (2025), refs 32-35.
Case reports of cancer developing or worsening after vaccination, Gibo et al. (2025), refs 26-41.
The Australian Institute of Health and Welfare is currently working off projections for rates of cancer mortality (2023-2024) and incidence (2021-2024).
As of the end of 2023, 80% of the Japanese population had received their first and second doses, and 67%, 46%, 30%, 20%, and 13% had received their third, fourth, fifth, sixth, and seventh doses.
An excess 3,870 (95%CI: 1,739, 5,989) in 2021, 7,162 (4,786, 9,522) in 2022, and 4,729 (2,110, 7,327) in 2023 for all cancers.
Influence of multiple modRNA Covid vaccinations, Gibo et al.(2025), refs 32-33 and 42-56.
Thrombogenic effects of spike protein and LNPs, Gibo et al. (2025), refs 57-72.
Suppression of cancer immunosurveillance, Gibo et al. (2025), refs 73-83.
Possible effects of spike protein on development and progression of specific cancers, Gibo et al. (2025), refs 45 and 84-100.
Concerns regarding effects of residual DNA fragments on development and progression of cancer, Gibo et al. (2025), refs 101-114.
Ironically, the original preprint which is actually identical to the 2024 peer-reviewed paper retracted by Cureus remains on the Zenodo server.
What made it far worse for me as an observer, but moreso for Cancer patients, was that during the hysteria, Cancer therapy was refused until jabbed.
This whole post it, then retract it, proves powerful people are pulling strings, and we the public must be quick to note, download and distribute new information, to bypass their efforts at censorship.
But it also means that there are good people doing their best inside - allowing the posting, knowing full well the inevitable takedown to come after. And maybe hoping that people like you notice and carry on after they are silenced.
The flip side of this is the quality of journal articles that so get published and don't get retracted.
Having been reading medical journal paprs for over 40 years, I have witnessed the descent into a mire of pseudo-scientific waffle, hopeless conflicts of interest, peer review that has completely lost its original meaning, and journals that don't even attempt to hide their Big Pharma love fest.
Unfortunately it's now a case of caveat emptor.
Or as I said to my registrar yesterday, eat well, exercise, and get plenty of fresh air!