
3 months of NSW data show it's not the unvaccinated in hospitals with Covid
The argument for Collective Good is on shaky ground

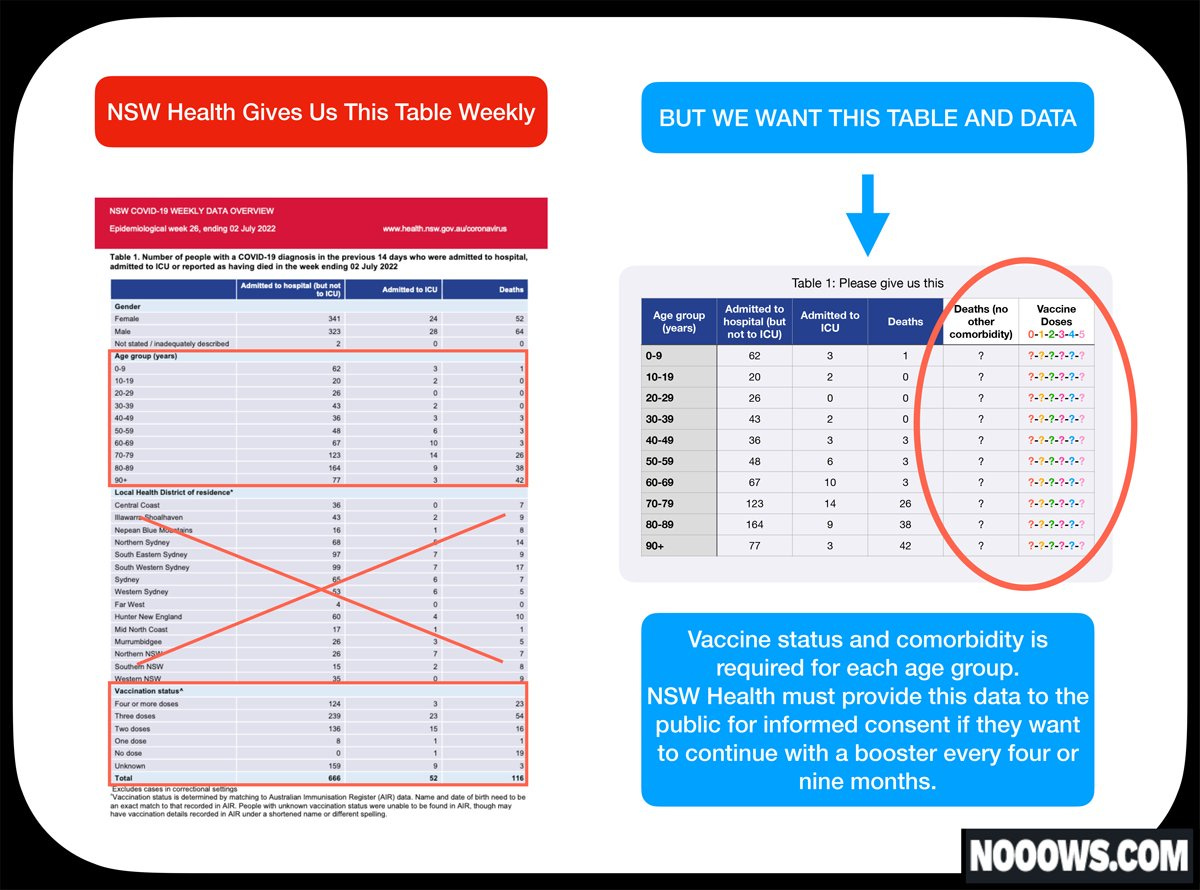
Is NSW Health aware that there are barely any unvaccinated patients being hospitalised with Covid? In last week’s Covid surveillance report, there were 0 (zero) unvaccinated patients hospitalised with Covid. In the past 3 months, there was a grand total of 21 unvaccinated patients (0.2%) out of a total 9, 348 Covid hospitalisations.
I’ll let that sink in.
The remaining 9, 327 is comprised of:
4+ dosed (1, 935),
3 dosed (3, 274),
2 dosed (1, 762),
1 dosed (122),
Unknown (2, 234).
NSW Minister for Health Brad Hazzard’s vaccinations may be up to date, but unfortunately, his Covid FAQs are not.
Incidentally, the NSW Covid FAQs are out of date in more ways than one. They state that vaccinated people have less chance of catching and spreading Covid, but the latest NSW booster drive campaign exemplifies the messaging pivot we are seeing nationally and internationally. Government and health officials are moving away from ‘Vaccines protect the community by preventing infection and transmission’ to, ‘Vaccines protect the community by preventing hospitalisation. Save our hospitals!’.
Sneaky of NSW Health to use the phrase “may not always stop you catching COVID-19” instead of the more truthful ‘won’t stop you catching COVID-19.’I want to get into the data so I won’t get bogged down in the transmission/infection prevention narrative, but I mention it here to highlight that public messaging has moved on from the idea that vaccines prevent infection, or transmission, and this is significant for reasons which I will explain in the conclusion.
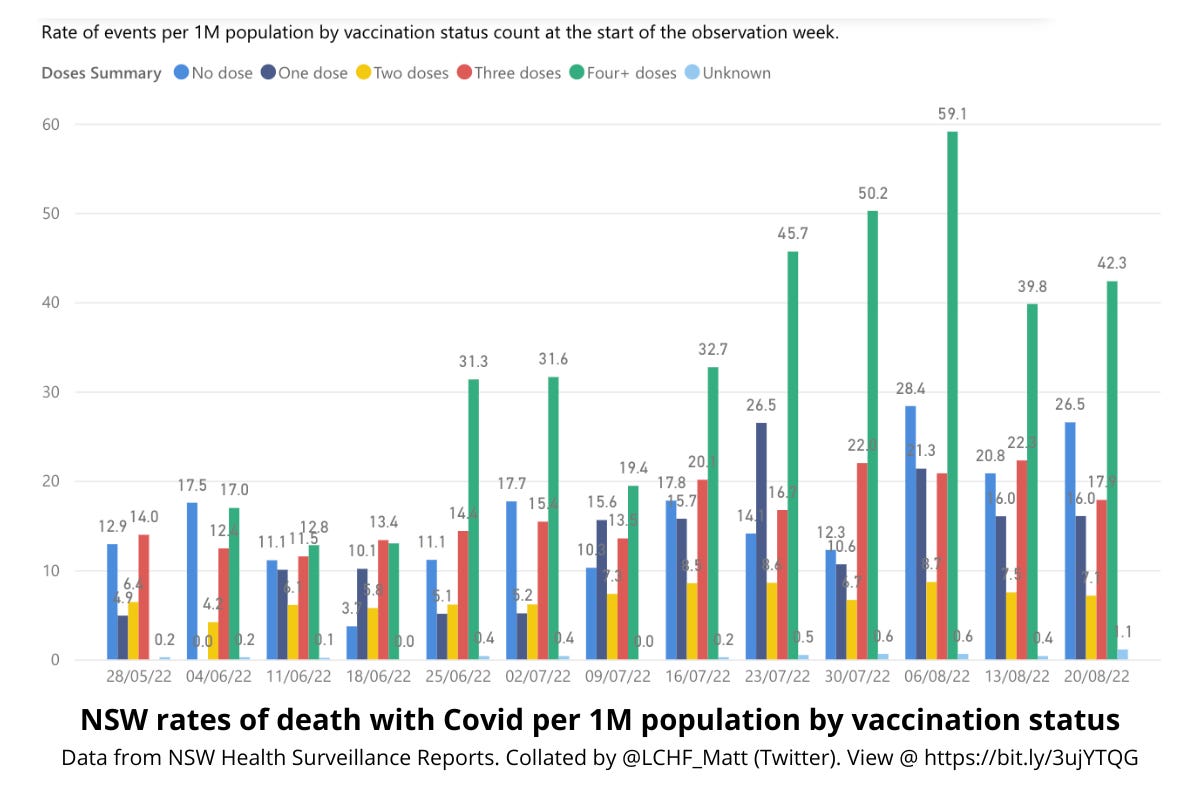
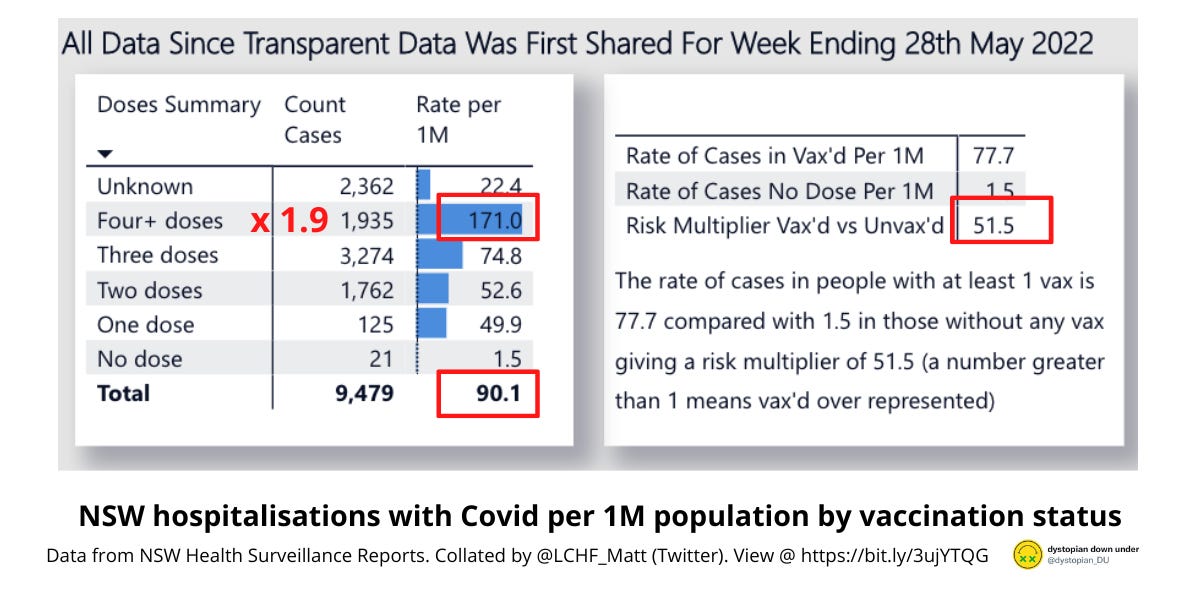
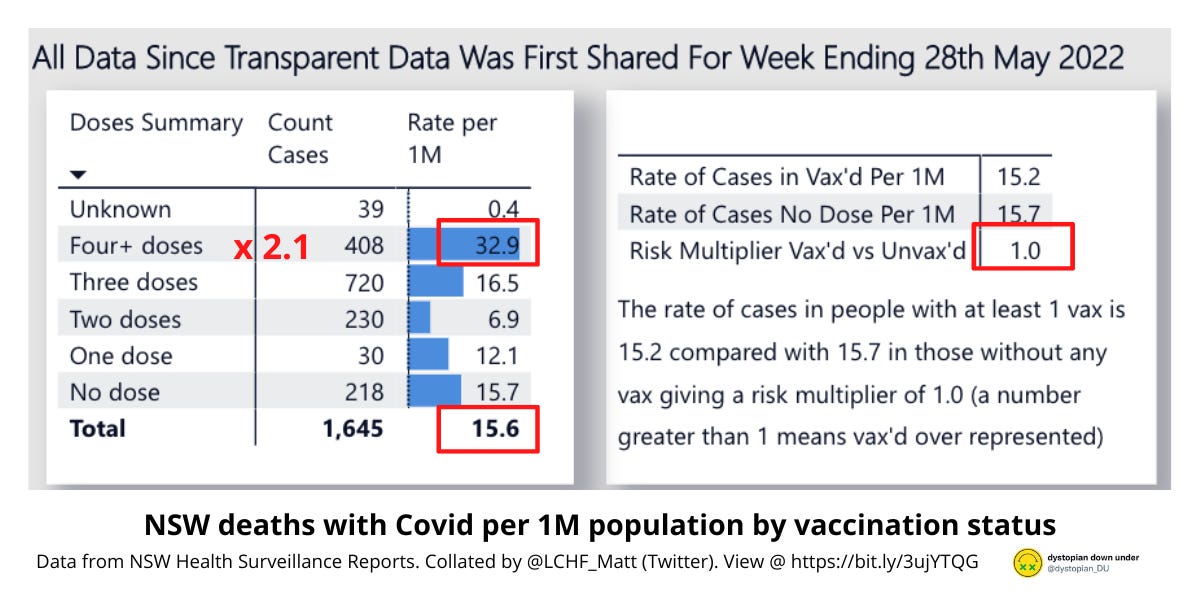
It’s 3 months, or a full quarter, since NSW reverted to publishing the full breakdown of ‘with Covid’ hospitalisations and deaths by vaccination dosage. Twitter user @LCHF_Matt has put his data skills to good use in creating this data sheet, which allows us to view the rate of hospitalisations and deaths with Covid by vaccination status, week by week. The below graphs show cases by vaccination status count on a per 1M population basis (total measured events divided by the count of the population with that vaccination dosage x 1 million), which allows us to see the rate of hospitalisation and death for each group relative to the proportion of the population that shares the same dosage status. This is important, because viewing raw numbers does not account for the fact that the majority of the NSW population has now received one or more dose of Covid vaccination.

OBSERVATIONS
1. Per the headline, there are barely any unvaccinated people in hospital with Covid. The risk multiplier for vaccinated vs. unvaccinated is 51.5, meaning that it is 51.5 times more likely that a patient hospitalised with Covid is vaccinated than unvaccinated. The 4+ dosed group is over represented by a factor of 1.9 in with Covid hospitalisations.
2. The 4+ dose group is also over represented in deaths by a factor of 2.1. The 3 dose group is over represented, but by a much slimmer margin. The risk multiplier for vaccinated vs. unvaccinated with Covid deaths is 1, which means that the unvaccinated are represented in Covid deaths to the same proportion that they are represented in the general population.
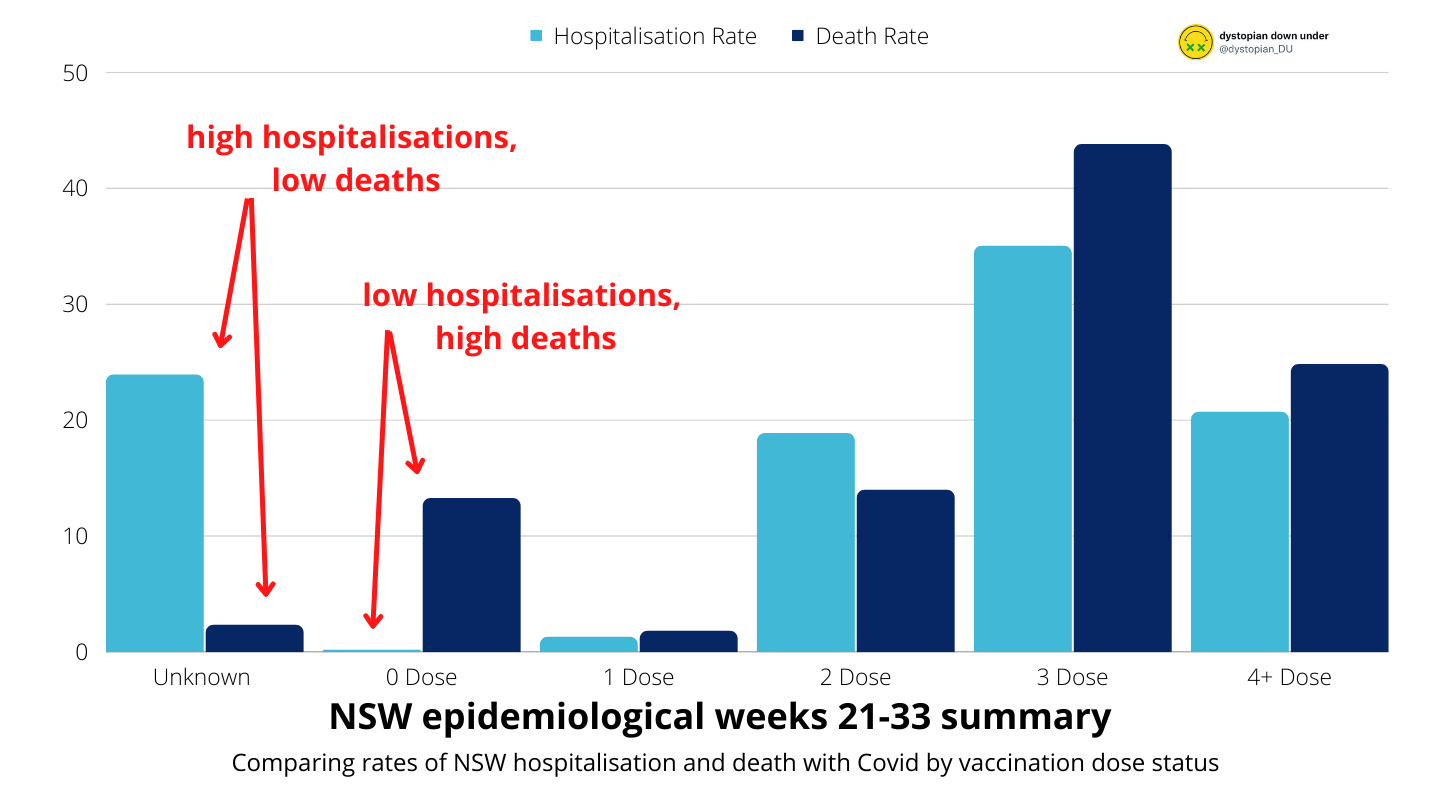
3. Unknown vaccination cases make 23.9% of hospitalisations but only 2.4% of deaths. Why? It seems strange that NSW Health cannot determine the vaccination status of nearly ¼ hospitalisations, but they can do so for almost all deaths. At the same time, only 0.2% of hospitalisations are 0 dosed, yet this group makes up 13.25% of deaths. In the other groups (1, 2 and 3 doses) the rate of death tracks more closely to the rate hospitalisation. See the below graph comparing rates of with Covid hospitalisation (bright blue) against deaths (navy) over combined epidemiological weeks 21-33. The disparity between the high hospitalisation rate and low death rate of Unknowns against the low hospitalisation rate and higher death rate of 0 dosed is striking.
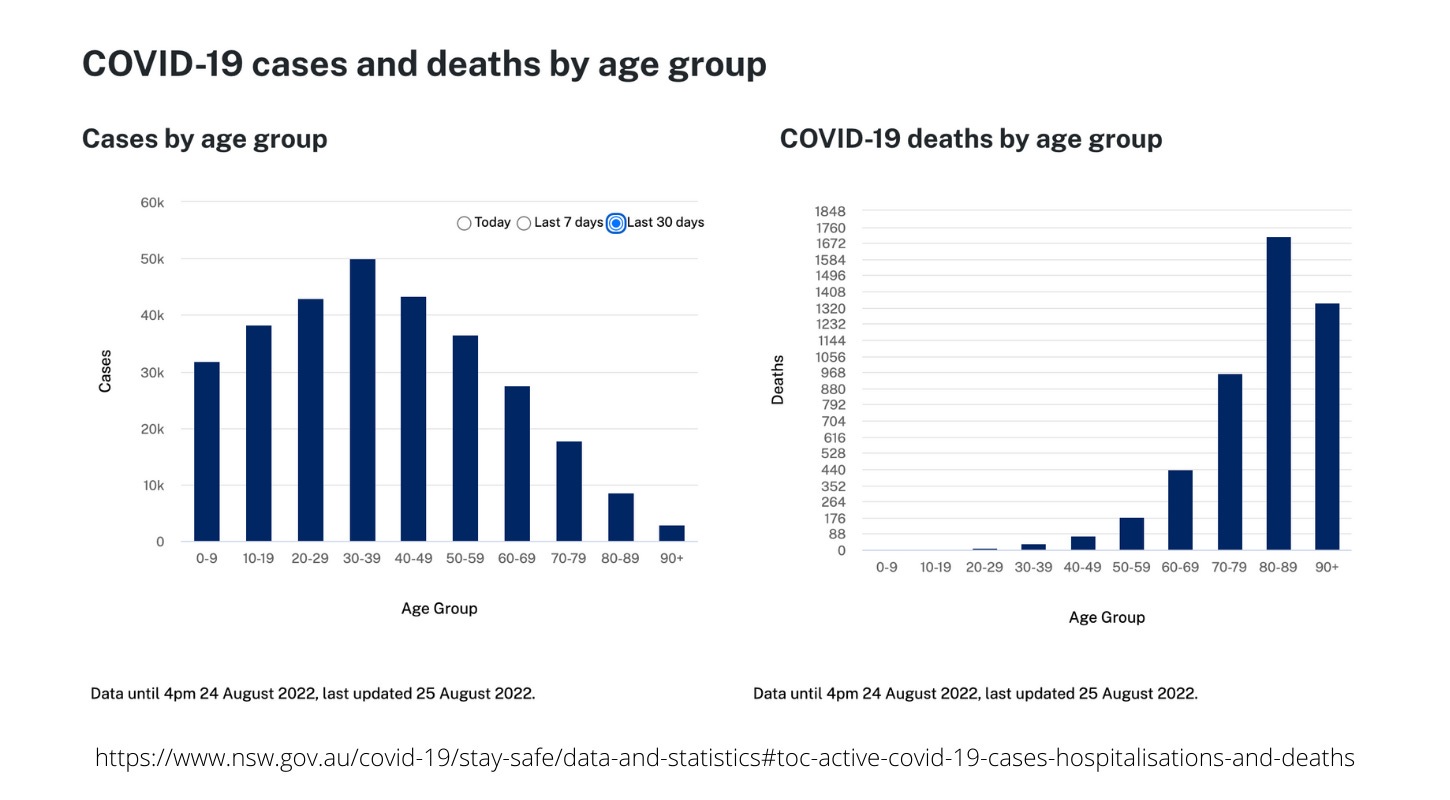
4. Covid cases in NSW are more prevalent in younger age groups, whereas Covid deaths are overwhelmingly occurring in the 70+ age group. The below chart shows NSW case data from the past 30 days compared with cumulative NSW Covid deaths from the beginning of the pandemic until 25 August 2022. The ratio of deaths shown below mirrors what we see from the past 13 weeks of surveillance data.
Additional observations from the NSW surveillance reports
(which can all be found HERE)
5. Aged care deaths account for 774/1645 deaths with Covid from this period, or 47%.
6. 77/1645 of deaths with Covid occurred at home.
7. For weeks 21-30, NSW Health gave a tally of the number of deaths with Covid under the age of 65. During this 10 week period, there were 76 deaths with Covid in the under 65 group (4.6% of total deaths). 73/76 of these people (96%) were reported to have died with significant comorbidities. From weeks 31 onwards, NSW Health stops reporting on the number of deaths under 65 and on associated comorbidities.
DISCUSSION
From 3 months of NSW Covid surveillance reporting, we can see that higher rates of hospitalisation and death with Covid correlate with higher dosage rates of Covid vaccination.
We see the same correlation of increased hospitalisations/deaths with increased doses of Covid vaccine bearing out in other parts of the world also. See: the Netherlands; USA; Canada; Israel; NZ; Portugal.
But – everyone say it with me – correlation does not necessarily mean causation! Let’s scratch a bit further.
Death with Covid is predominantly affecting the aged. Less than 5% of deaths with Covid occurred in those under age 65 during the period that NSW reported for this age bracket, and 47% of deaths with Covid occurred in aged care facilities.
Comorbidity appears to be another significant factor in death with Covid. Of those who died with Covid under age 65, 96% died with significant comorbidities. National figures from the Australian Bureau of Statistics (ABS) show that Covid is recorded as the sole cause of death for just 5.3% of deaths with Covid. The remainder of the deaths involve either causal sequences, such as pneumonia caused by Covid, or comorbidities, which are pre-existing chronic illnesses. The ABS lists chronic cardiac conditions, dementia, chronic respiratory conditions, diabetes, cancer, kidney disease, and hypertension as the most common comorbidities for death with Covid.
The authors of the Great Barrington Declaration (GBD) pointed out the higher risk to the aged and infirm almost two years ago:

SOURCE
The GBD was dismissed by mainstream media and governments as ‘fringe’ science. Formerly lauded professors from the 'fringe' institutions of Harvard, Stanford and Oxford were ignored, and Covid was declared a deadly risk and an equal level of threat to each and every person. However, current NSW data support the GBD position on this.
There is the argument that the aged and infirm are more likely to have had more doses of Covid vaccine, and that this explains the over representation in deaths and hospitalisations in the higher dosed groups. It may be the case that the elderly, immunocompromised and terminally ill have more boosters than younger people on balance. After all, these groups are typically given access to new doses earlier than the general population, and ATAGI has recommended the fourth and even a fifth dose to the more vulnerable members of our population. Having said that, it’s also possible that some elderly and ill are too frail to take the primary or booster doses. If this is the case, it may go part way to explaining why 0 dosed deaths are proportionally much higher than 0 dosed hospitalisations – if they are unvaccinated elderly people dying in aged care, they never counted as a hospitalisation case before passing.
Regardless, Covid vaccines are supposed to reduce the severity of illness and the likelihood of death, so if the vaccines work as stated, one might reasonably expect the rates of hospitalisation and death in the most highly vaccinated to drop off, or at least be neutralised.
Counter! Covid is so deadly that the vaccines are working, and if everyone hadn’t taken them, there would be even more deaths and hospitalisations.
Counter to the counter! Then why aren’t there way more unvaccinated people in hospital and dying with Covid? If the vaccines are improving outcomes for the 87% of the NSW population who has taken them, and yet these people are still over represented in hospitalisation and death (which they are), then we should see the 0 dosed overwhelmingly, unequivocally, absolutely drowning the hospitals and mortuaries with severe illness and death. We’re not seeing that. Further, if the high rates of 3 and 4+ dosed people being hospitalised and dying with Covid is proof that Covid is so deadly that even 4 vaccine doses can’t prevent hospitalisation and death, then we should see ungodly numbers of hospitalisations and deaths with Covid reported for countries with low vaccination take up when controlling for other factors.
I note that it is a common error to interpret data that suggests poor real-world effectiveness for Covid vaccines against Omicron and subsequent variants only in light of trials showing efficacy against Wuhan and Delta strains. I have added a brief explainer under Bonus Content at the end on the difference between vaccine efficacy and vaccine effectiveness. If people want to claim that the vaccines have high effectiveness despite the boosted being over represented in hospitalisations and deaths with Covid, the burden of proof is on them to either conduct, or reference, rigorous reporting comparing hospitalisations and deaths with Covid in highly vaccinated countries to countries with low vaccination take up. If you have links to such reports, please post in the comments and I’ll read them. It’s one of the tangents that I’m currently researching.
None of this can be settled without better data, such as age stratification by dosage for hospitalisation and deaths, and reinfection rates by dosage. It is very difficult to do anything other than speculate on causal factors, and thus the above discussion should be taken as speculation.
What we can state with confidence though, is that if you’re in hospital in NSW with Covid, it’s highly likely that you’re vaccinated, boosted, and boosted again.
We should talk about the Unknown group, because it makes up nearly 1/4 of hospitalisations. Who are they, and why are there so numerous in hospital but relatively few in deaths? Some say that Unknowns are all 0 dosed. Some say they are all vaccinated. In fact, their status is Unknown. The group can conceivably include a mix of vaccinated and unvaccinated people, as status is determined by matching the given name and date of birth to a record in the Australian Immunisation Register (AIR). Records that may not show up in AIR: anyone who has moved but not updated their address; misspells a name; has changed their name (eg: marriage); is not an Australian resident; received a non-approved vaccine overseas; received an approved vaccine overseas but has not applied to have it added to AIR; has never received a vaccination of any type and therefore has no AIR record.

SOURCE
It’s strange that NSW Health cannot identify the vaccination status for nearly 1/4 of hospitalisations, yet can manage the distinction for all but 2.4% of deaths. Proof of vaccination (POV) is still in place for working and visiting aged and disability care settings in NSW. If staff at an aged care facility can identify whether a visitor is vaccinated or not (via the approved forms of POV), how is it that hospital staff cannot? Dr Ah Kahn Syed makes a strong case for data fixing. I don’t know the answer, but as Unknowns are unknown, I have treated them as such in this discussion.
Throughout the pandemic, health officials, politicians and media outlets have dishonestly lumped Unknowns with 0 dosed when reporting on hospitalisations and deaths with Covid. I covered this in detail in my post, How to lie with statistics. For the sake of the argument, however, I did an experiment. I added all the Unknown hospitalisations and deaths with Covid to the 0 dose count for the past 3 months. Pictured in the graph below, the proportion of hospitalisations (aqua) and deaths (navy) with Covid against the proportion of the population with the relevant dosage (magenta).
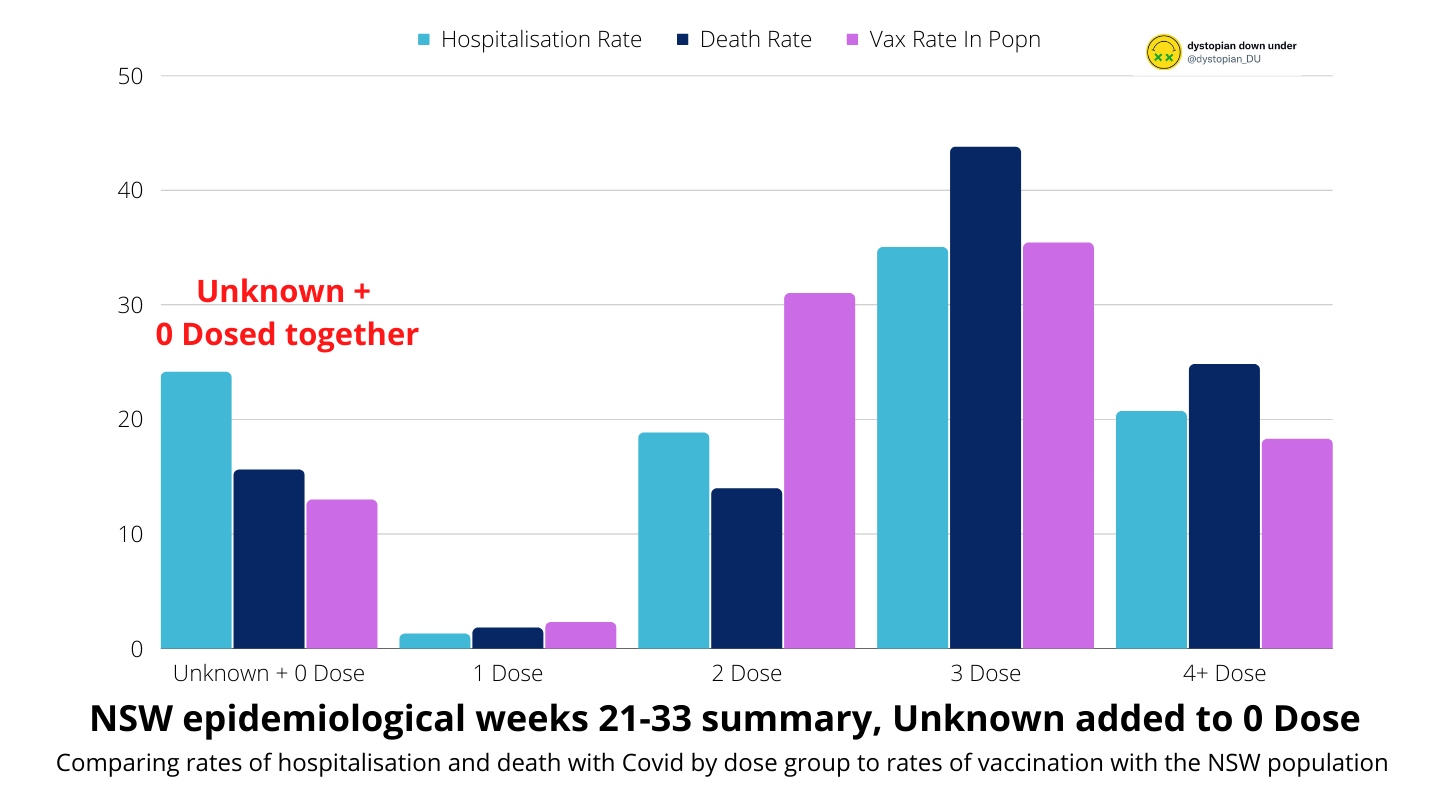
In this hypothetical scenario, the 3 and 4+ dose group are still over represented in hospitalisations (4+ dosed) and deaths (3 dosed and 4+ dosed) with Covid. In this experiment, 0 Dosed would also be over represented in hospitalisations and in deaths. The experiment is unrealistic, as it’s highly improbable that the Unknown group is homogeneous. Nevertheless, the point is to highlight that even in the extremely unlikely event that all Unknowns were 0 dosed, the 3 and 4+ dosed groups are still suffering disproportionately high rates of hospitalisation and deaths with Covid. Thus, even if we are to accept the dishonest framing employed by politicians and the media, NSW Covid data raises serious question marks over whether the Covid vaccines are able to keep people from being hospitalised and dying in any meaningful way.
CONCLUSION
NSW Covid data from the past 3 months show that:
a) There are hardly any unvaccinated people in hospital;
b) Neither are unvaccinated people disproportionately dying with Covid, and;
c) The 4+ dosed groups are over represented in hospitalisations and deaths with Covid, with the 3 dosed highly represented in both as well.
This is huge. These data threaten to cut the last cord holding together the argument for Collective Good that is the sole and necessary foundation for measures such as vaccination mandates, passports, and restrictive and punitive measures applied to unvaccinated citizens.

First, they told us that these measures were necessary in order to prevent infection and transmission of a deadly virus, for the Collective Good. Then, when it became patently obvious that the double boosted were getting infected as much as the 0 dosed, they told us that these measures were still necessary to ease the burden on the healthcare system, for the Collective Good.
But if the unvaccinated are not the ones taking all the hospital beds, or the ventilators, then vaccination is simply a personal health choice, like eating organic veg, or losing weight, or quitting cigarettes. And if vaccination is a personal health choice with no social good other than one’s own potentially improved well-being and satisfaction in taking it, then we would have to reconsider everything.
The workplace mandates.
The constant media coverage on vaccination efforts.
The enormous portion of the state and national budgets dedicated to vaccines, roll outs and associated services.
The punitive measures being taken against the 0 dosed.
And our governments and health bodies would owe some MAJOR apologies to the unjabbed.
Families prevented from visiting aged parents, even on their death beds.
Parents not allowed to stay with their newborn baby in hospital.
Workers put on leave without pay or dismissed from their jobs.
Workers subject to disciplinary action and docking of pay.
People ex-communicated from their families, disinvited to Christmas and birthdays.
Families separated from each other for months across state lines, while the vaccinated traveled freely across borders.
But our governments and health bodies would owe the biggest apology to the vaccinated.
The ones who took it willingly were misled to believe that the manifold promised benefits would eventuate. To the ones who were coerced, the government would have to admit that there was never any good reason for the coercion; it was only abuse. These people took the vaccine purely to keep their jobs, or to see their mother in another country, to visit their dad in aged care, or to go to the gym because their mental health depended on it. These people accepted the gross expenditure on vaccination programs and the diversion of primary healthcare resources to vaccine rollout, because the government told them it would save them, their families and the hospitals. Many of these people comforted themselves with the mantra that at least they would not burden the healthcare system. At least they were doing their bit. But the truth hurts. They were coerced by their own government on false grounds.
WHERE TO FROM HERE
NSW Covid data should sound the alarm for the media to start doing their job. That is, holding truth to power. While mainstream media outlets have consistently declined to do their job over the past two years, preferring instead to publish barely edited press releases on behalf of government and giant pharma companies, the tide does appear to be turning as far as commentary on pandemic management goes. We may see a few more brave journalists follow the lead of Australian journalists like Andrew Bolt (The Bolt Report), Rita Panahi (Sky News), Rowan Dean (The Spectator), Frank Chung (news.com.au), and Chris Uhlmann (Nine News). I hope so.
We should see a call for better data, and better transparency in the sharing of this data, so that collectively we can make sense of the situation unfolding in Australia at the moment.
It is encouraging to see a few mainstream media items from recent weeks highlighting the shortcomings of the published Covid data. For example, The West Australian, in a rare show of journalism (they usually stick to PR for powerful entities), reported last week that 2/3 of hospitalisations with Covid at Fiona Stanley Hospital were actually there for reasons other than Covid.
Channel 9 reported that just 10% of WA with Covid deaths were of Covid.
How many NSW hospitalisations and deaths are of Covid? We don’t know. We will need the mainstream media to apply strong pressure to federal and state governments and health bodies to get them to keep and release better data, as is their duty to the public who pays them.
In the meantime, the data that we do have is enough to call what’s left of the threadbare Collective Good argument into question. There should be vigorous and urgent parliamentary and public debate over the appropriateness of vaccination mandates and passports, and associated restrictions and punitive measures. If it turns out that the Collective Good argument has no basis (and it looks like it’s going to fall that way), journalists and media outlets will want to be on the right side of history. They can ensure that they are by asking the tough questions, now; by putting these issues front and centre on the news agenda; by investigating government attempts at obfuscation; and by sharing their findings with the public.
BONUS CONTENT
If you want to deep dive on theories of causation (speculation) for the high representation of the 3 and 4+ dosed in hospitalisation and death with Covid, see my earlier post referencing the bad cat and Geert Vanden Bossche.

Vaccine effectiveness vs. vaccine efficacy
These two terms do not mean the same thing. Many lay people use them interchangeably, as did I until I recently learned the difference, but the distinction is important.
VACCINE EFFICACY: the measurement of how well a vaccine performs in a clinical trial against a placebo group.
VACCINE EFFECTIVENESS: the measurement of how well a vaccine performs in the real world.
Used in a sentence: “Despite showing promising efficacy in clinical trials, the Covid vaccines have shown poor effectiveness since rollout in the population.”
GAVI has a neat little explainer page on the difference between the two terms, HERE.
On prevention of transmission and infection, some recent developments:
Aus Health has removed all mention of infection or transmission prevention from its How COVID-19 Vaccines Work page.
Victorian Chief Health Officer Brett Sutton has publicly stated that, “Despite 2, 3, 4 doses of the vaccine, it’s not so good at preventing infection in the first place.”
The CDC has updated its Covid advice to now treat vaccinated and unvaccinated people who have been exposed to Covid as sharing the same infectiousness risk profile.
https://roundingtheearth.substack.com/p/reanalysis-of-the-society-of-actuaries?r=uao93&utm_medium=ios
The brilliant statistician Mathew Crawford makes a compelling argument for zero vax efficacy and instead that wealth is the main factor determining outcomes. It and his other many articles diving deep into the US data are some of the best I’ve come across throughout the plandemonium
just on statistics ....
Have the CDC, FDA, the WHO or even our very own CSIRO or any other scientific or academic labs on this planet in the last 2.5 years ever have a isolated sars cov 2 ( the virus ) that causes covid 19 ?
THE ANSWER IS NO
No one has ever seen it and no records exist.
https://www.fluoridefreepeel.ca/68-health-science-institutions-globally-all-failed-to-cite-even-1-record-of-sars-cov-2-purification-by-anyone-anywhere-ever/
Literally hundreds linked to this page