
My Body, My Choice
On reproductive rights, vaccine refusal, and cognitive dissonance

The My Body, My Choice gang is back in town and they're here to sort the pro-choice wheat from the anti-vax chaff.
The pro-choice/pro-mandate crowd have worked themselves into a twisted state this week and in order to provide a robust rebuttal, it does take a while to methodically unravel the pretzel. I’m going to use the term ‘woke-choicers’ to refer to the pro-choice/pro-mandate camp as it’s less of a mouthful and I prefer to steer clear of pejorative pro- and anti-vax labels. Woke-choicers are different to classical pro-choicers in that they apply their pro-choice philosophy selectively, generally in line with where public sentiment falls on woke issues. I want to acknowledge the existence of a third group who take the pro-life/anti-mandate position. As I am focussed on rebutting the attacks of woke-choicers on classical pro-choicers over their use of My Body, My Choice, I will not make any further mention of this group in the following essay.
I wrote this rebuttal because I’m angry about being attacked by people who I’m standing with and for. But more importantly, I wrote it because the division and hate I’m seeing online (and spilling into offline conversations) is so unnecessary. Enough with the bickering. We can identify our common ground and stand together in unity or we can burn the whole house down while we’re in it. I choose the former and I hope you do too.
Roe v. Wade has been overturned. Everyone has an opinion. Cue, woke-choicer telling everyone how to behave, with this pearler from Dr Matt Agnew.
”My body my choice being co-opted by the anti-vax crowd is utterly deplorable, disgustingly hurtful and tremendously dangerous.”
Similar diatribes are making the rounds, like this article and this one from the Gates Foundation-funded Gavi Vaccine Alliance. They all follow a similar two point plan, with colouring in around the edges.
My Body, My Choice only applies to abortion rights, and anyone who uses it under any other circumstances is wrong, especially immoral anti-vaxxers.
Abortions only involve the woman having it. Refusing a vaccine endangers everyone. Therefore these issues are not comparable and the classical pro-choicers who fight for bodily autonomy on both these issues are not just wrong, they’re biological terrorists.
If I were an Independent Fact Checker I would flag the first point with a context warning: only partially true. The slogan My Body, My Choice has been used all over the world for decades in relation to women’s bodily autonomy including the right to work, to fair wages, to own property, to education, and to reproductive rights. The slogan is also associated with class struggles and men’s circumcision activism. To suggest that My Body, My Choice is a slogan exclusively dedicated to the advocacy of abortion is historically inaccurate. I would also be interested to know how woke-choicers think that men, people without uteruses, and classical pro-choice women ought to express their desire for bodily autonomy. My Biology, My Autonomy just doesn’t have the same oomph. This argument is splitting hairs. Or are woke-choicers actually saying that women who wish to abort foetuses are the only category of human beings on earth who have the right to bodily autonomy at all? It’s such an absurd claim that I’ll give the benefit of the doubt and assume that when woke-choicers berate classical pro-choicers for applying My Body, My Choice without discrimination, it is because they are hung up on slogan rights.
The second point takes some more unpacking.
’Abortions only involve the woman but anti-vaxxers endanger everyone.’
Firstly, and problematic use of ‘anti-vaxxers’ aside, this statement misses the entire crux of the pro-life argument, which is that you exercising your right to bodily autonomy necessarily ends the life of another person. You might disagree, but to pretend that this argument, this perceived harm does not exist is dishonest. It’s a point that Richard Dawkins elucidates in this article, They Think it’s Murder.
It’s worth considering the worst case scenario of each camp.
Pro-lifers think the worst outcome is the murder of a baby, and they think that the worst outcome happens in every single case of abortion. As Dawkins points out, to pro-lifers, every year we are undergoing, “an annual holocaust of hideous magnitude.” The counter argument is that the foetus is just a clump of cells. To accommodate the broadest view of the pro-life argument, we can say that to pro-lifers, abortion constitutes anything from bloody murder to truncating a life that, without interference, would otherwise have progressed.
Woke-choicers think the worst outcome is that an ‘unvaxxed deplorable’ will give them or someone they love Covid. In this worst case scenario, there is a small chance that the person will die. The risk is lower for people under 65, higher if you’re over 65 or have a high number of comorbidities. (This Oxford University calculator tool provides evidence-based calculations for a range of risk factors including age, vaccination status, ethnicity and comorbidities. My risk of catching and dying from Covid is 0.002%. I caught Covid and lived, which was 99.998% likely). Woke-choicers also fear that Covid infection via an unvaccinated person will put them at risk of developing long Covid symptoms. As almost everyone gets Covid anyway, one has to question whether it matters exactly who they get it from (I address transmission further down in points 1. and 2.). But to woke-choicers it really matters whether they get it in January via an unvaccinated person or in February via a vaccinated person, and as we are considering the worst case scenario of each camp, I will entertain the concern.
Side by side, the worst case scenario of a pro-lifer is infinitely more terrible than that of the woke-choicer. It’s a life-ending trade off every time. The woke-choicer’s worst case is statistically much less likely, and in most cases will not involve the ending of a life (clump of cells, fully formed human or otherwise). To say that abortions only affect the woman but anti-vaxxers endanger everyone is to completely ignore the concerns of one camp and at the same time inflate beyond proportion the concerns of the other camp.
The inverse of this argument goes something like,
‘To equate vaccination to the inability of a child who has been raped to access an abortion is hurtful and obscene.’
This argument labours under a logical fallacy - that of comparing the most extreme worst-case scenario of anti-abortion law with the best-case scenario of vaccine mandates. The most extreme case of suffering from illegal abortion is forced birth of a rapist’s child, or the death of a woman trying to obtain an illegal abortion. The most extreme case of coerced vaccination is death, or permanent disability. Both of these worst-case scenarios are emotionally devastating, life-ruining, horrific. ^(see end notes for comment on the rate of extreme cases)
That the flawed logic behind comparing rape victims to happy and willing vaccinees is so easily dismantled raises the question - why then do so many people fall for the error? I suggest that media censorship has everything to do with this. If you read, you know the attendant suffering that anti-abortion laws produce. Umpteen thought pieces circulate daily painting just the picture. The suffering of vaccine injury victims, however, is highly self-censored in legacy media and is aggressively censored by big tech on social networks. Because the emotional and physical carnage wreaked by vaccine mandates is largely censored, it remains unseen. In the instances that posts concerning vaccine injury are not flagged and removed, they are delegitimised by context warnings declaring the vaccines to be safe.

I am not aware of routine red flagging, or context warnings on social media for sharing information on the pitfalls of anti-abortion law, even in the cases of obvious misinformation. Are you? Some legacy publications cover the negative fall out of anti-abortion law more than others, but I do not see the wholesale silencing of discussion on this topic in legacy media the way that we see it on the topic of vaccine injury. (Listen to UK journalist Sally Beck discuss the extreme and unusual nature of Covid related censorship in this podcast with fellow journalist James Delingpole).
Any fair debate involving extreme worst cases must compare worst to worst. In reality, the extreme worst cases of illegal abortion and of vaccine mandates are both awful. Classical pro-choicers acknowledge this, and seek legal protection for both groups of potential victims. Woke-choicers find themselves in the contrary position of advocating for one class of victims while ignoring or gaslighting the other class of victims. They also blow their own fears out of proportion while at the same time minimising or, again, simply ignoring the fears of their philosophical opponents.
Thus far I have focused mainly on the first half of the claim that, ’Abortions only involve the woman but anti-vaxxers endanger everyone’. Now to the second half of the claim, ‘that not receiving a vaccine endangers EVERYONE’.
This claim is predicated on 5 ideas:
The vaccines are sterilising (stops infection and stops transmission)
That by coming into contact with an unvaccinated d person, the other is necessarily at greater risk
The vaccines are safe
The vaccines are more beneficial than any other alternative
If 1, 2, 3 & 4 hold, it is then reasonable for the state to conscript your body in service to others
These ideas are the oxygen to the dumpster fire of anti-vax rhetoric raging through the online social sphere of late. Let’s see if they hold up to a light prodding.
1. The vaccine is sterilising (stops infection and stops transmission).
Very few vaccines are sterilising. The opposite of a sterilising vaccine is a leaky vaccine, which allows for both infection and transmission. The mandates up for debate recently involve leaky Covid-19 vaccines. That the Covid-19 vaccines are leaky is so far beyond obvious now it’s embarrassing to see anyone arguing against this fact, but we can perhaps excuse people who don’t read much. Remember, the narrative went from ‘One in 5,000 is the real chance of breakthrough infection’ in September 2021 (The New York Times) to ‘Few vaccines prevent infection but it doesn’t matter anyway’ in January 2022 (ABC). Now we’re at something like ‘The vaccines don’t prevent, limit or reduce infection or transmission, but thank Big Pharma for my booster or it would have been worse,’ a là twice boosted Canadian Prime Minister Justin Trudeau announcing his second Covid infection.
Some experts believe that leaky vaccines drive infection and new variants. Dr Geert Vanden Bossche is one who I’ve previously referenced on this issue. You can watch and read his plea to the WHO to stop vaccinating against omicron here.
There is also the problem of vaccine-derived outbreaks. This 2020 article reports vaccine-derived outbreaks of polio in Sudan, Chad, Pakistan and Afghanistan. Vaccine-derived polio has also appeared in London as of last week. Naturally, officials recommend getting vaccinated to prevent this vaccine-derived illness.
Statement 1 does not hold. Let’s move on.
2. By coming into contact with an unvaccinated person, the other is necessarily at greater risk.
For a leaky vaccine this is virtually a null point. Some claim that leaky vaccines allow infection but increase the likelihood of being asymptomatic, therefore reducing the viral load and decreasing the likelihood of you passing on the virus. Two problems with this claim:
a) Asymptomatic people are more likely to mingle in the community, spreading the virus unknowingly. Symptomatic people stay home. And,
b) The real world data do not support the hypothesis.
In highly vaccinated populations, we consistently see correlation with high rates of infection. See: Australia / Israel / UK / NZ / Portugal / Germany
This statement makes the error of assuming that vaccines are the only way of limiting spread of a disease. In Africa, where many nations having been using Ivermectin as a malaria prophylactic for years, they saw low rates of Covid-19 infection. Ivermectin was used to successfully treat Covid all over the world.
This statement also assumes that no test does or will exist that would determine whether the offender is contagious - bear in mind that most people are NOT contagious, most of the time. Further, this point overlooks the fact that decades of pandemic research and policy agrees that focused protection is the appropriate response to the vulnerability of the elderly, and that the main factor in bad covid outcomes aside from age is entirely within the individual’s control (obesity / weight loss).
Aside from this statement being largely dependent on point 1 (which did not hold), it’s wobbly on its own merits.
3. The vaccines are safe
What a doozy.
There is a gushing firehose of egregious safety issues.
This could just about be summed up in one picture of CDC data (which the CDC has just been forced under FOIA to admit to not having monitored AT ALL for safety signals).
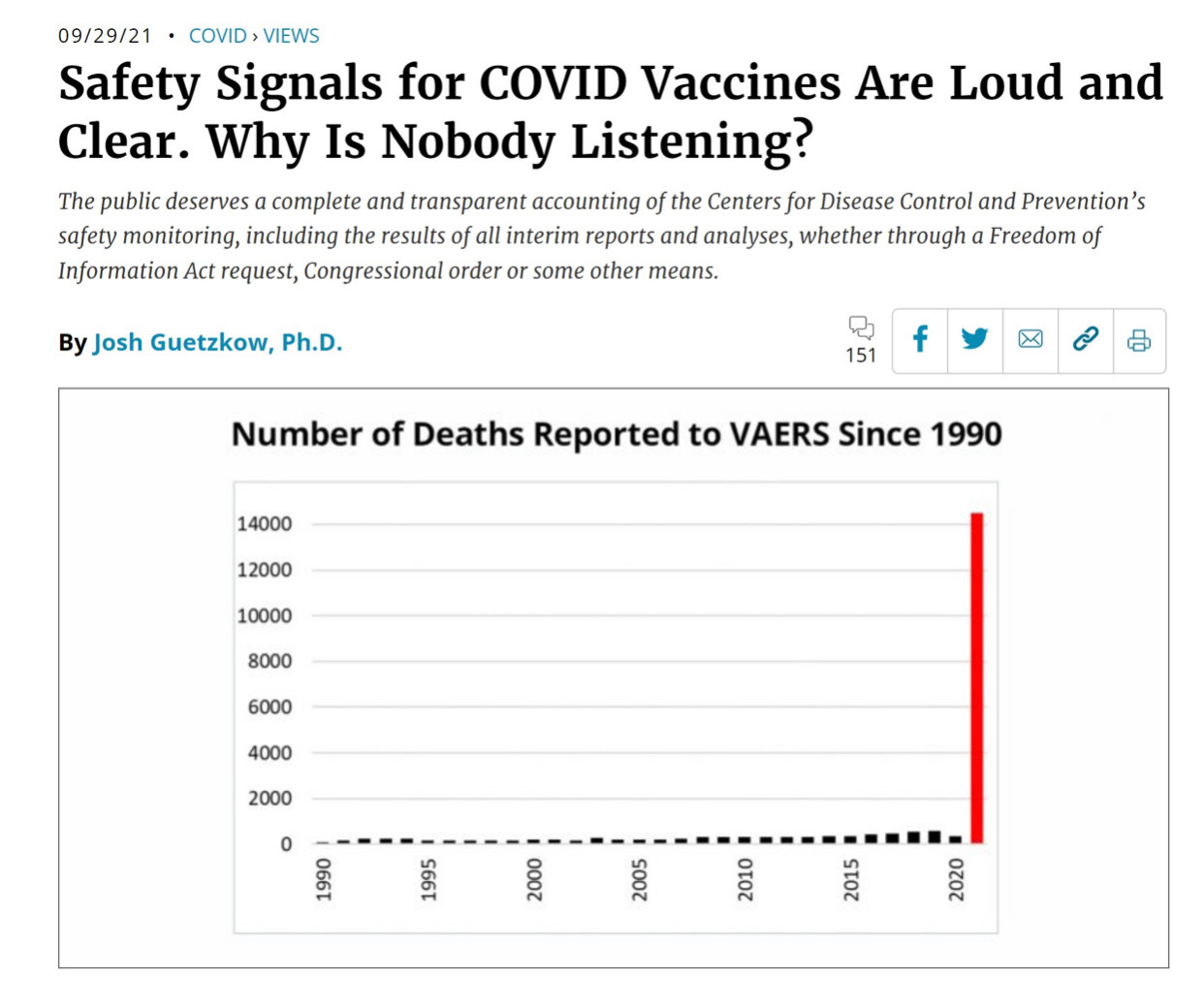
SOURCE
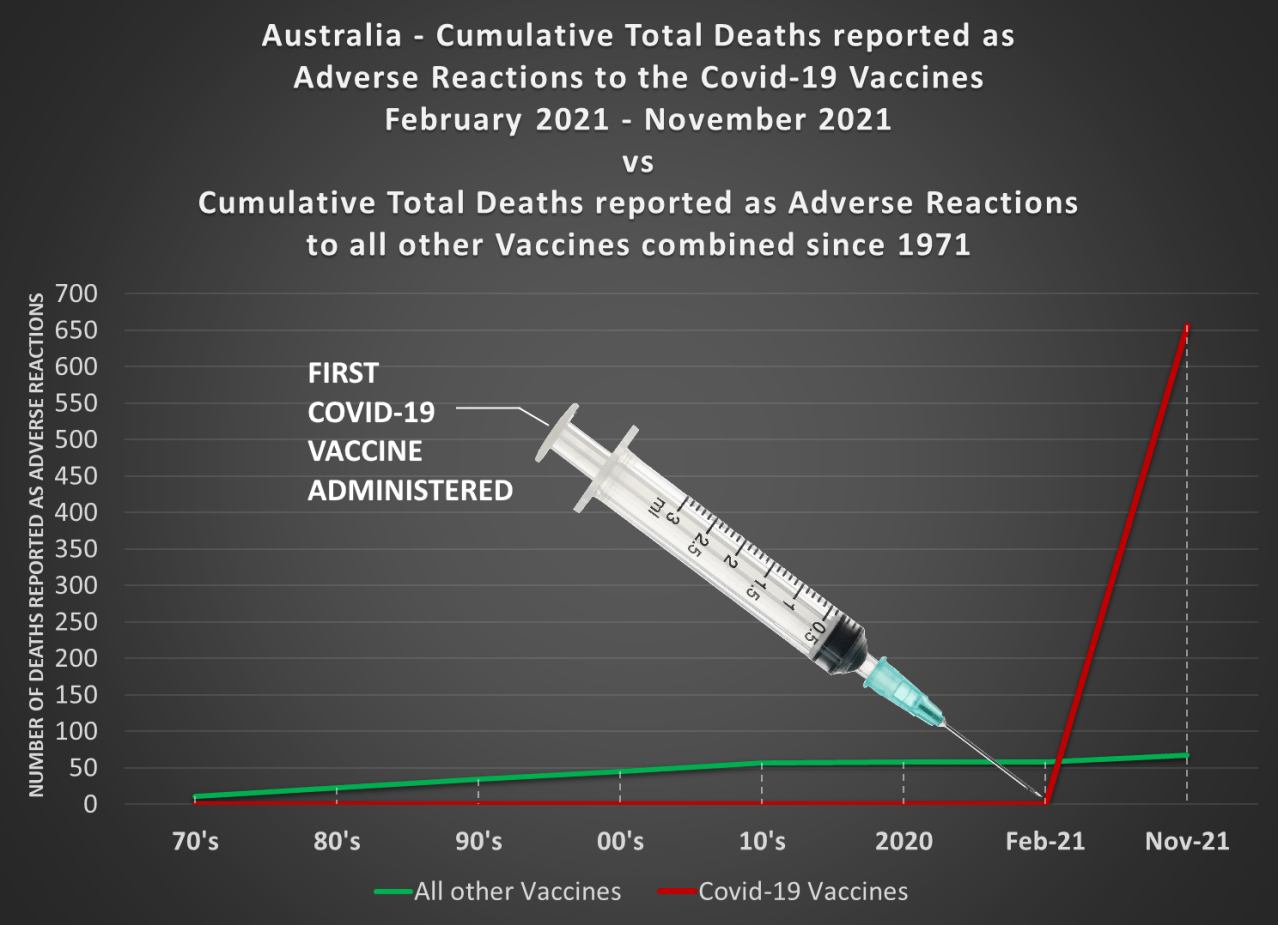
The Australian version doesn’t look good either. There have been 11 times as many deaths reported as adverse reactions to the Covid-19 vaccines over 8 short months than deaths reported as adverse reactions to every other available vaccine combined over a period of 50 years.
Here is a table showing some other variables of interest, including permanent disabilities, number of hospitalisations, and number of life-threatening events. The Covid-19 vaccines take first prize in every category bar one, and that’s compared to all other vaccines combined since 1990.
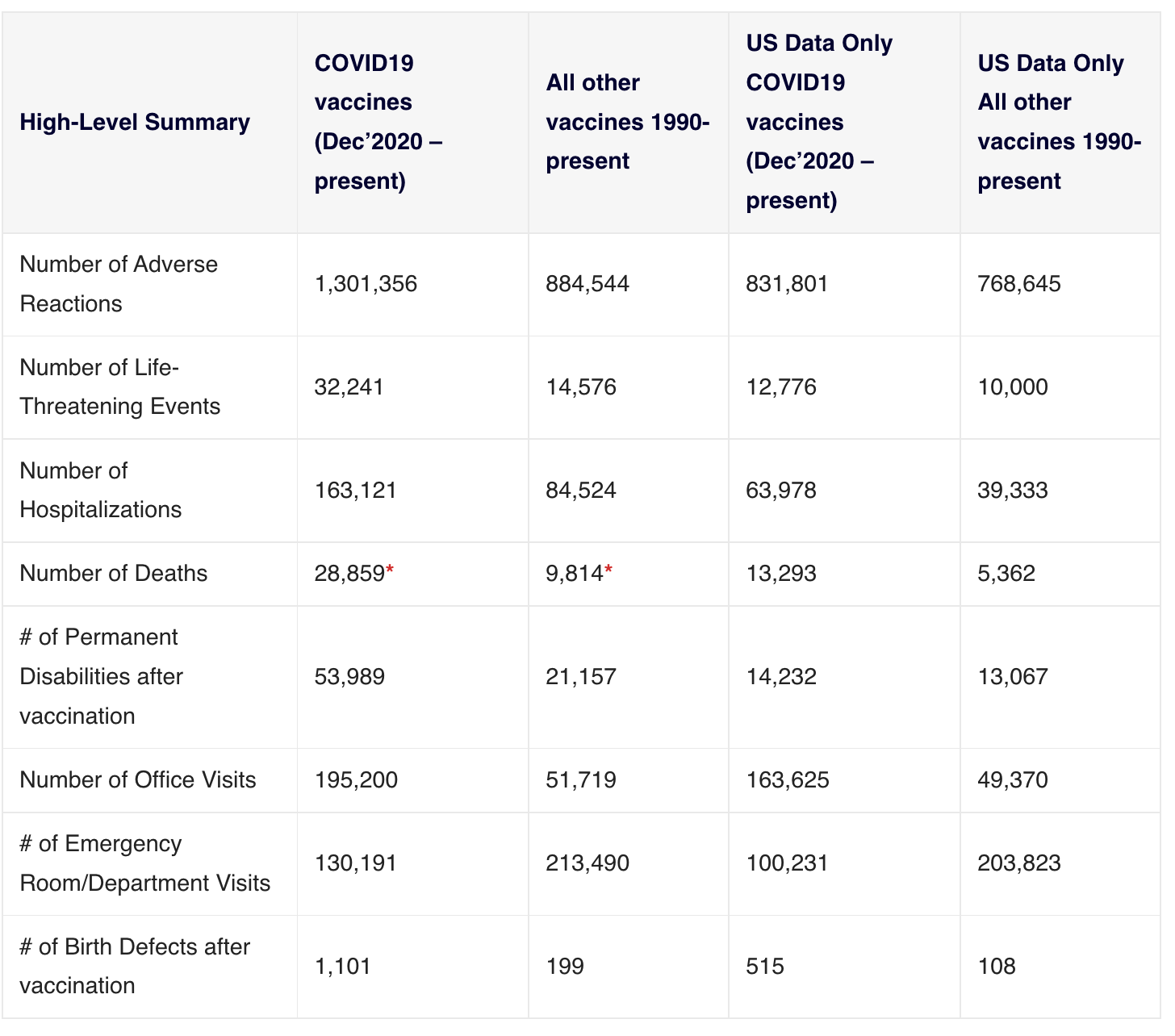
SOURCE
*A note on VAERS - VAERS is the foundation of the US vaccine safety monitoring infrastructure. Since the Covid vaccines starting causing such enormous spikes in VAERS reporting, there have been a number of debunking style articles published warning that anti-vaxxers will twist the data to show anything they like. For this reason, I prefer to read VAERS data analysis from qualified data analysts like Jessica Rose. However, even the debunkers agree that VAERS was established to pick up safety signals, and it is meant to be monitored closely by regulatory bodies. As mentioned above, it now turns out that the CDC has not been doing any such monitoring, despite the abundant and loud safety signals. And keep in mind that passive reporting systems like VAERS pick up only a small number of reports compared to the whole. IMOP has a good round up of the evidence for underreporting of adverse events. Queries over the authenticity of VAERS reporting also must be balanced by the knowledge that knowingly making a false report is a federal offence, punishable by fine and imprisonment.
But there’s so much more.
Brianne Dressen founded vaccine injury support not-for-profit React 19 in partnership with injured MDs and PhDs after her participation in the Astra Zeneca Covid-19 trial left her horrifically injured. Dressen’s injury occurred after the first dose, so she had to withdraw from the trial, which required two doses. Therefore, her severe adverse reaction was not included in the trial report, and Dressen was not eligible for medical or financial support from either AZ or the US government. The concerns around safety are not limited to the injuries themselves - they include the barriers and gaslighting that the injured face in seeking medical and financial help to recover.
People seem to think that the promise of ‘rare’ severe side effects make these vaccines safe. Well, they’re not safe to the people in the ‘rare’ category. Philosophical question - is it ok to require someone else be permanently disabled in order to reduce the likelihood of your grandma contracting Covid (assuming the vaccines would prevent transmission, which they don’t)? The victims who I interview for the Jab Injuries Global archive project don’t think so. Neither do their parents, grandparents, spouses or children. In some cases we interview the parent or partner, because the victim is dead.
And anyway, serious side effects are not actually so rare. Dr Naomi Wolf reports on the extensive harms to pregnant women and babies from Pfizer’s own documented trial results. It’s mortifying (probably don’t read it if you’re vaccinated and pregnant or breastfeeding, it will just be upsetting). She references the work of Etana Hecht, who also writes prolifically on this subject.
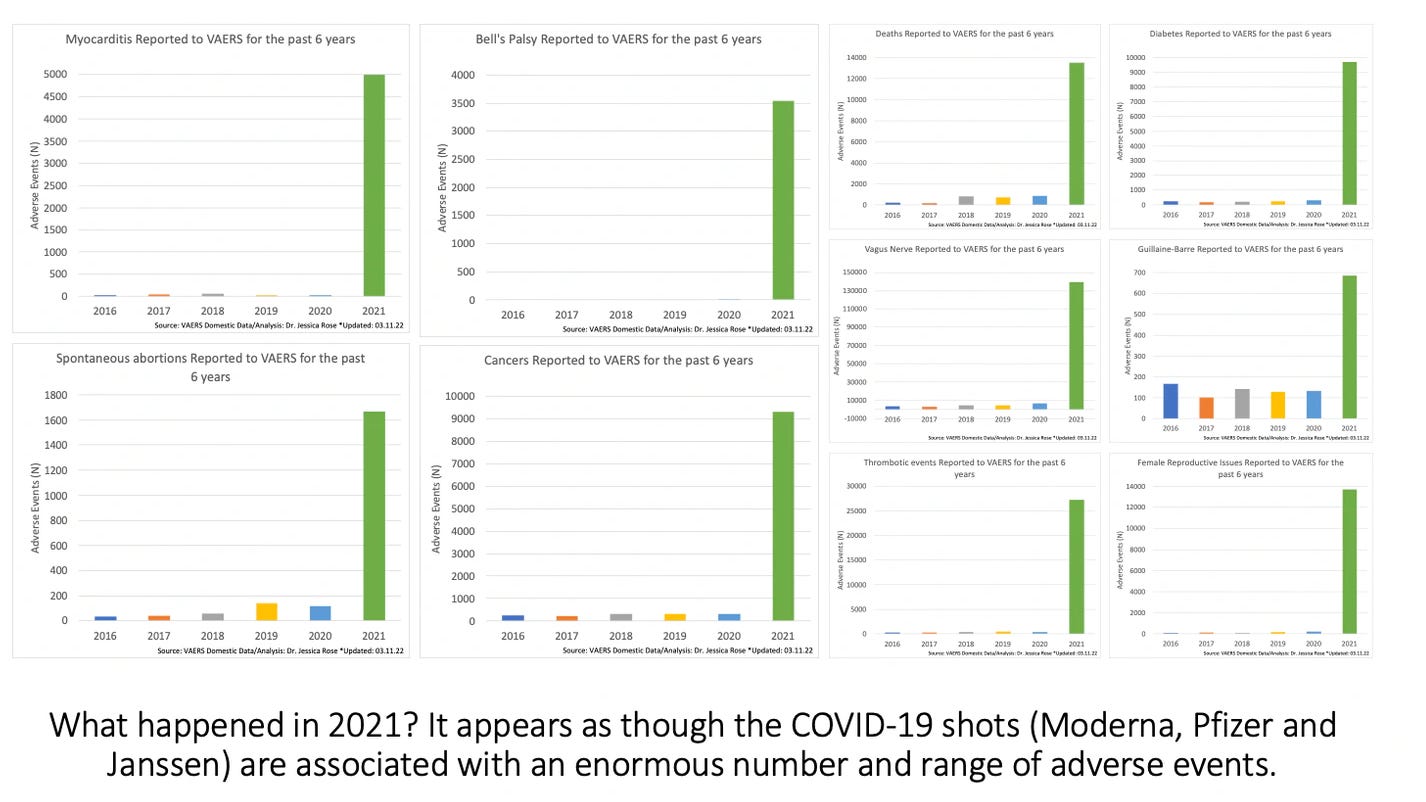
Dr Jessica Rose reports extensively on safety issues. Her data analysis skills are excellent.
Some European countries have banned Moderna for under 30s due to the “very rare” risk of myocarditis from the vaccine in this age group - so rare that they needed to ban the vaccine in that age group. This study across 4 Nordic countries compared myocarditis incidence in vaccinated but uninfected vs. unvaccinated but previously Covid infected groups. They found that incidence of myocarditis is higher in the vaccinated (uninfected) group than in infected (unvaccinated) group, especially in males 16-24.
I’ll leave it there. There are enough question marks over the issue of safety to, at the very least, park it until someone can properly explain what the hell all those safety signals are about. It would help if they can bring those jab injury victims back from the dead also.
4. The vaccines are more beneficial than any other alternative
Let’s say that the vaccines do afford benefit. Compared to what? Certain treatments have been documented again and again as providing astounding results for the end points of reduced severity of illness and reduced deaths. Dr Tess Lawrie, co-founder of the British Ivermectin Recommendation Development Group (BIRD) reports that Ivermectin is shown to reduce Covid-19 deaths by an average of 68% and to reduce Covid infections by an average of 86%. In this submission of evidence to UK parliament she summarises the body of evidence to date. The Front Line Covid-19 Critical Care Alliance (FLCCC) also links to a tonne of such studies. Incidentally, one of the founders of the FLCCC is ICU physician Paul Marik, who is preeminent in his field and has a resume a mile long. In the following video he chokes back tears as he says,
”We know these fucking vaccines cause at least 2-3% of people who get them will have adverse events like you’ve just heard (sic)… This is a humanitarian crisis.”
I am yet to find any rigorous, well-documented comparison of vaccine treatment vs. other treatment. If anyone has seen one, please comment.
UNSW Professor and Economist Gigi Foster put together what I believe is Australia’s only cost benefit analysis for lockdowns and border closures, which showed a 36:1 cost to benefit ratio in QALYs and WELLBYs. I’ve not seen one for Covid-19 vaccines produced by our government yet, have you? If so, again, please comment. It is the responsibility of the government to provide a cost-benefit analysis to the public in matters as far reaching as this, especially if it is the premise on which the government sees fit to withdraw basic rights (such as freedom of movement or the right to work).
This point is unsupported at this stage. That leaves one last point to address.
5. If 1, 2, 3 & 4 hold, it is then reasonable for the state to conscript your body in service to others.
They don’t hold. But for the sake of the thought experiment, let’s imagine that they do.
The great philosophical question that rages on in matters of conscription to war, conscription to forced birth and conscription to vaccination is, can the state reasonably conscript bodies to the service of others, and if so, what do the public require in return? Margaret Atwood posed this eloquently in a letter she wrote to an Argentinian news outlet when Argentina banned abortion in 2018. Atwood suggested that governments seeking to conscript men into war or women into childbirth ought to provide clothing, food, shelter and other amenities. Currently, the only thing provided to vaccinees by the Australian government is a Covid-19 claims scheme should you be severely injured, one that is notoriously difficult to qualify for.
Agnew and Co. say that pregnant women who want to abort their foetuses (or even fully formed babies) are the only people who have the right to this discussion, this negotiation with the government over whether their bodies should or should not be conscripted. Agnew’s reasoning is that vaccination is a choice, while being denied access to legal abortion removes women’s choice. Huh. Let me ask you this,
If a woman could receive an abortion, but in doing so she must forego her right to work, to cross state border lines, to sit in the hospital with her mother or to enter her university - would you SERIOUSLY champion her government for giving her a CHOICE?
I didn’t think so. It’s a ridiculous position to take. And yet Agnew and the woke-choice brigade are seriously suggesting that is fair and reasonable for the government to withdraw one’s right to work, to freedom of movement, to access education and amenities and so on, as penalty for exercising one’s right to bodily autonomy.
Being coerced into giving up one’s bodily autonomy (vaccination) in exchange for the right to work is not a fair choice, just as having to get on a bus to go to a state that will let you get your abortion, or having to source abortion pills on the black market severely curtails a woman’s choice in exercising her bodily autonomy. Woke-choicers’ insistence that mandated vaccination affords choice while illegal abortion removes choice reveals myopic dedication to a blatant double standard.
And it is this double standard that undermines any productive discussion of the question, is it reasonable for the state to conscript your body in service to others?
Pro-choice abortion advocates say no.
Pro-lifers say yes.
Pro-choice vaccination advocates say no.
Pro-mandate advocates say yes.
There is significant cognitive dissonance at play in the way we approach bodily autonomy in relation to different topics. It’s worth taking this opportunity to revisit the facts, and work through the logic one point at a time. Holding our ideas up to scrutiny and daylight is always a good thing. As John Stuart Mill reminds us in that foundational democratic treatise On Liberty - at the very least your argument will be strengthened in the process.
^ Extreme, or ‘hard’ abortion cases make up approximately 3.5% of abortions in the US. The rate of extreme Covid-19 adverse events (AEs) is hard to quantify due to regulatory body malpractice and the systemic failure of doctors to appropriately asses and document injury (such as this case and this case). Data analyst Dr Jessica Rose (her qualifications include immunology and applied mathematics) reports a 1/324 (3%) AE rate for Covid-19 vaccines. World renowned ICU physician Paul Marik estimates a 2-3% severe AE rate (see embedded video under point 4.).
BONUS CONTENT
On the issue of Roe V. Wade, my personal opinion mirrors that of Naomi Wolf fairly closely. You can read her reasonable and compassionate take below.
BONUS BONUS CONTENT
20 Bold Takes on the Roe Draft Opinion, The Atlantic
Hey. Thanks so much for this post. I was taken with your transparency and openness in the comments of the Bad Cattitude Substack today (14 April) I will add to that discussion but wanted to affirm you as you travel in search of reality, and felt like I needed to come read the source material.
Wish I had your ability to express myself so clearly. Really great points you put forward here! Not an easy topic to address. I have been in the camps of anti-mandate, anti-abortion (with some medical exceptions), pro-life and the cognitive dissonance is real as you say. The idea of conscription of body makes me deeply uncomfortable. The truth is, that is the nature of pregnancy... It is a type of conscription. It's burdensome, it's not always convenient, it can be traumatic and life threatening... And when you stop observing and valuing the miracle that life is, it can fast become ugly. In war, soldiers are painted in shades of glory and society is encouraged to revere their bravery. For some, this makes the daunting task more bearable. It can help with loss and grief among soldiers and family. I think that's what bothers me about the pro-abortion argument and what has pushed me further into other camps. We have lost sight of the wonder that is new life - in any form - and the deep profound admiration of women for bearing the weight of it all. Society is failing women if they feel they need to have an abortion, and women are failing women for pushing such a pessimistic outlook instead of building each other up and offering ongoing practical community support. And I mean real hands-on community, not State Daddy bullshit.