
A vaccine that can kill you even if you don't take it. Wait, what?!

Well this is terrifying.
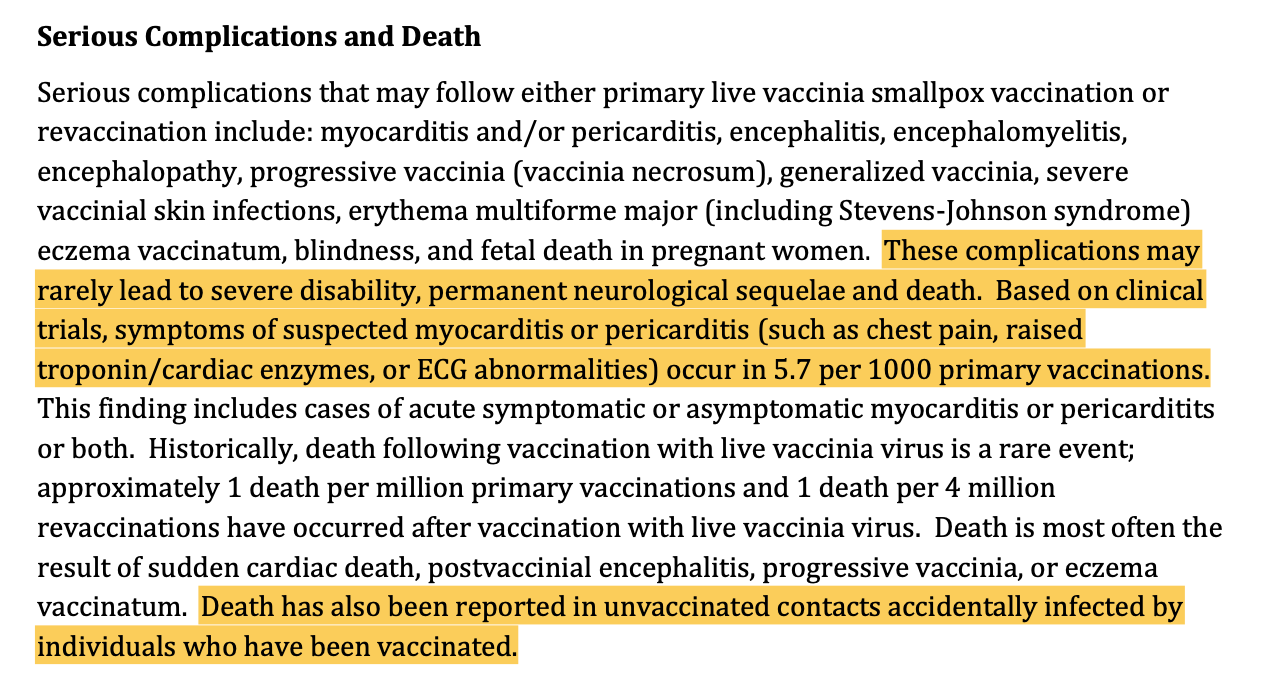
ACAM2000 is one of two smallpox vaccines approved for emergency use (EUA) in treatment of Monkeypox (MPX) in Australia. It can cause death to people who come into contact with vaccinees. See the below from page 6 of the ACAM2000 product info sheet:
SOURCE
Note that risk of death to unvaccinated contacts is not mentioned on the accompanying Consumer Info Sheet provided by the TGA. It appears that the TGA considers rare risks to be negligible.
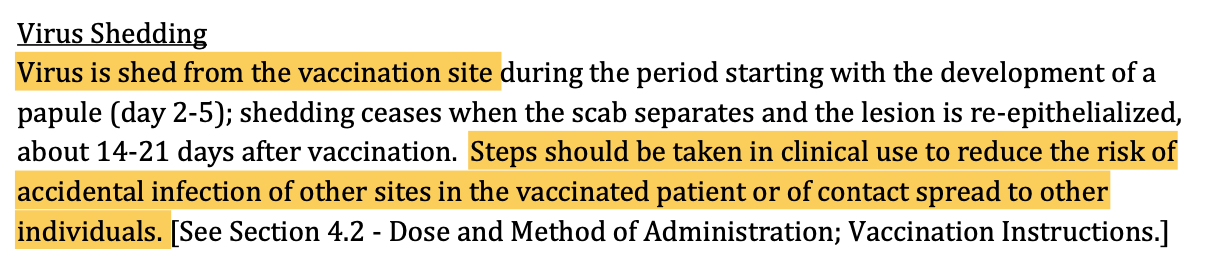
As I understand it, the reason that unvaccinated people are at risk of side effects of ACAM2000 is that the vaccine uses live-attenuated virus, which means that vaccinees shed for a period of time after vaccination (sources generally agree on a window of up to 3 weeks after vaccination, or until scabbing at the injection site has healed). I could be wrong on my understanding of the causal mechanism for ACAM2000 side effects to unvaccinated contacts. If anyone reading this is qualified to speak in more detail on the shedding of live-attenuated virus from vaccinees to unvaccinated contacts and the associated risks, please add to the comments below. Nevertheless, we can say with certainty that ACAM2000 results in shedding of the MPX virus from the site of vaccination, because the product sheet tells us on page 17 that this is so:
SOURCE
This raises important ethical questions around the use of the ACAM2000 live-attenuated virus vaccine.
Naturally, vaccinees can and should take steps to minimise the possibility of shedding live virus to unvaccinated people. The TGA consumer information sheet recommends not touching babies or sharing a bed and linens with an unvaccinated person for the period after vaccination, but that’s as specific as it gets. Are vaccinees aware of the potentially grave effects of not taking seriously the precautions recommended in the consumer info sheet? Do doctors administering ACAM2000 impress upon vaccinees the danger to close contacts? Is anyone regulating what information is provided to vaccinees, in how much detail, and whether unvaccinated contacts are receiving the appropriate information also?
In light of the recent extreme responses of our state and federal governments to viral threat, it would be an interesting thought experiment to ask: should we treat vaccine virus shedding in the same manner that we treated Covid virus shedding early in the pandemic (ie: when cases were comparatively rare in the community, as is the current situation with MPX)?
During the early days of the Covid pandemic, you could be sent to prison for life for deliberately transmitting Covid to a healthcare worker. You could go to prison for up to 10 years for coughing on someone.
Should ACAM2000 vaccinees be subject to special laws under threat of life in prison if they knowingly shed to unvaccinated individuals? And if not, why not? It seems contradictory to threaten life in prison for knowingly spreading one virus but not another, especially if both viruses have Global Pandemic status. Covid has a higher death rate, so perhaps the penalty could be adjusted down to reflect the lower death rate of MPX. Then again, death is death to the person that dies from a virus, so one might argue that it is insult to the dead to issue a lower penalty for transmission of one virus over the other.
Perhaps penalties should only apply if the infected person is seriously injured or dies. Covid penalties applied simply for coughing or knowingly being in contact with another individual who then may or may not contract the virus, and who then may or may not get very sick and die. Perhaps these penalties should be applied according to patient outcome, not the act of contact.
Then again, virus shedding after ACAM2000 vaccination is transmitted through contact, so should we treat vaccine shedding the way that we treat other contact-based transmissions - like STI transmission? Laws around STI transmission vary from state to state in Australia, but as a rule, fines and imprisonment only apply where the act of transmission occurred due to wilful transmission, or failure of the infected party to take ‘reasonable precautions.’ In NSW, for example, you can be fined $11K and/or go to prison for 6 months for knowingly transmitting an STI. Note that, though rare, STIs can cause death.
The purpose of this thought experiment is to highlight the different ways in which viral* threats (from vaccines, from airborne exposure, or from contact) are managed by lawmakers. As it stands, it does not appear that there are any legal protections in place for unvaccinated contacts of ACAM2000 vaccine recipients. I also question whether ACAM2000 vaccine recipients are made properly aware of the potential harms to contacts from shedding during the weeks after vaccination. One would certainly hope so.
And what about JYNNEOS, the other smallpox vaccine that has EUA for treatment of MPX in Australia?
Only the ACAM2000 info sheet directly references the potential for death and other severe side effects to unvaccinated contacts. The JYNNEOS vaccine also contains live-attenuated virus, but I couldn’t find any specific mention of potential harms to unvaccinated contacts within any of the product information sheets via TGA or FDA websites.
Is this because JYNNEOS poses no risk to unvaccinated contacts, or is this because no testing has been conducting to determine whether unvaccinated contacts are at risk? I cannot find an answer to either question.
If ACAM2000 causes viral shedding from the site of vaccination, and this is associated with risks to unvaccinated contacts, then it seems logical that JYNNEOS will do the same, with similarly associated risks. However, as I am not expert enough to fully understand the mechanisms underlying vaccine shedding, or the differences between different types of live-attenuated vaccines, I cannot speak with clarity or certainty. What I can say is that, as a lay-person, it bothers me that these questions have not been addressed - at least not in such a way that is easy to locate or understand via product inserts, consumer info sheets, or via any Australian government or health agency websites.
To the skeptics who may counter with the claim, ”but these side effects are rare!” This is essentially the ‘jellybean roulette’ argument that was rather distastefully gamed out in the widely panned BBC documentary, Unvaccinated. The obvious answer to such an argument is that, in discussing risks associated with medical interventions, we are dealing with people, not jellybeans:

Where there is risk, there must be proper, informed consent. The implications of vaccine shedding effects on unvaccinated contacts must be part of this conversation. Where heath policy and laws protect individuals from wild virus shedding but not vaccine virus shedding, these contradictions should be assessed and rectified. We need to consider whether, as a society, we think that transmissible diseases and associated interventions should be managed socially, at the level of individual and community, or whether they should be managed legally, by state and federal governments. These are big questions. I’d love to see them parsed out in the public discourse.
FURTHER READING
Health Australia Monkeypox Info Page HERE
ATAGI Guidance on Vaccination Against Monkeypox HERE
ACAM2000 Product Info HERE
ACAM2000 Consumer Info Sheet HERE
RX LIST ACAM2000 Product Summary HERE
JYNNEOS Info Sheet HERE
RX LIST JYNNEOS Product Summary HERE
*Acknowledging that STIs can be viral or bacterial
Live UN-attenuated
Most dangerous